
Asymptomatic Carotid Bruit/Carotid Artery Stenosis
- There has been increased interest in using statins to slow the progression of carotid artery disease. In the Asymptomatic Carotid Artery Plaque Study, lovastatin was compared in a double-blinded study to evaluate the effect on intima-media thickness and cardiovascular events. In both men and women with moderately elevated low-density lipoprotein levels, the progression of intima-media thickness in the carotid arteries was reduced compared with placebo, and lovastatin was also associated with reduced cardiovascular events and mortality.
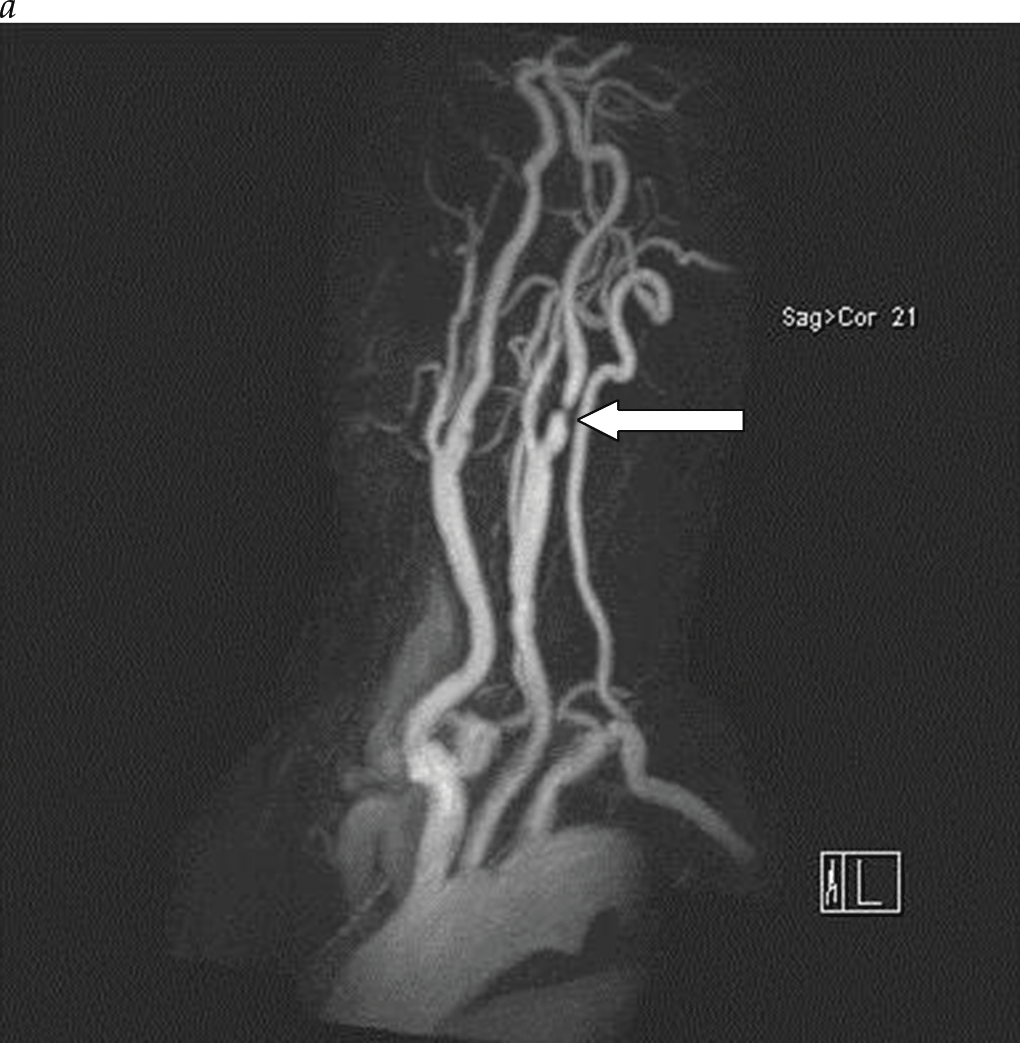
- The initial imaging study for patients with carotid bruit or cerebrovascular symptoms is duplex imaging of the extracranial carotid arteries. Duplex ultrasonography is an accurate and reliable noninvasive tool to determine the degree of carotid stenosis and plaque morphology in most patients.
- Conventional angiography, once considered the gold standard for carotid imaging, is now reserved for patients with conflicting studies or patients being considered for carotid stenting. Conventional contrast selective carotid angiography poses a stroke risk of approximately 1% and therefore has a limited role in place of modern MRA and CTA, except in cases of planned carotid stenting.














.png)

















