- The DSM-III ushered in the era of criteria-based diagnoses that improved the reliability of the psychiatric diagnostic process.
- The multiaxial diagnostic system was discontinued in the DSM-5 because it had outlived its usefulness and was subject to misuse.
- The DSM-5 emphasized the importance of dimensional assessment, although not as extensively as originally hoped.
Latest Updates


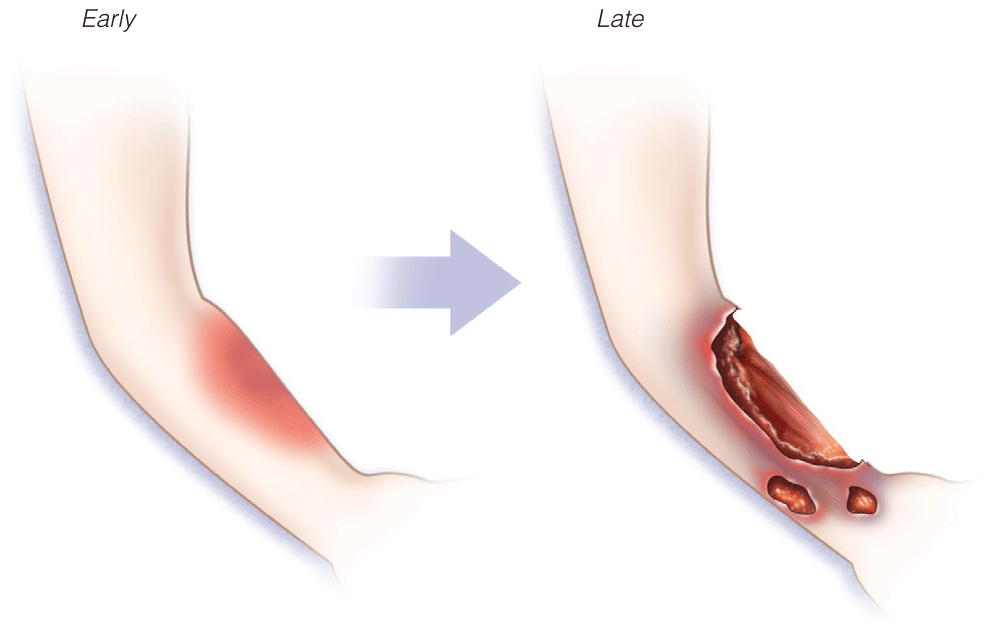
- Pediatric skin conditions are the third most common reason for presentation in the ED for children
- Suspected Rocky Mountain spotted fever should be treated immediately, before laboratory confirmation, as untreated cases can progress to serious illness or death
- Clinical scoring systems for necrotizing fasciitis and toxic epidermal necrolysis

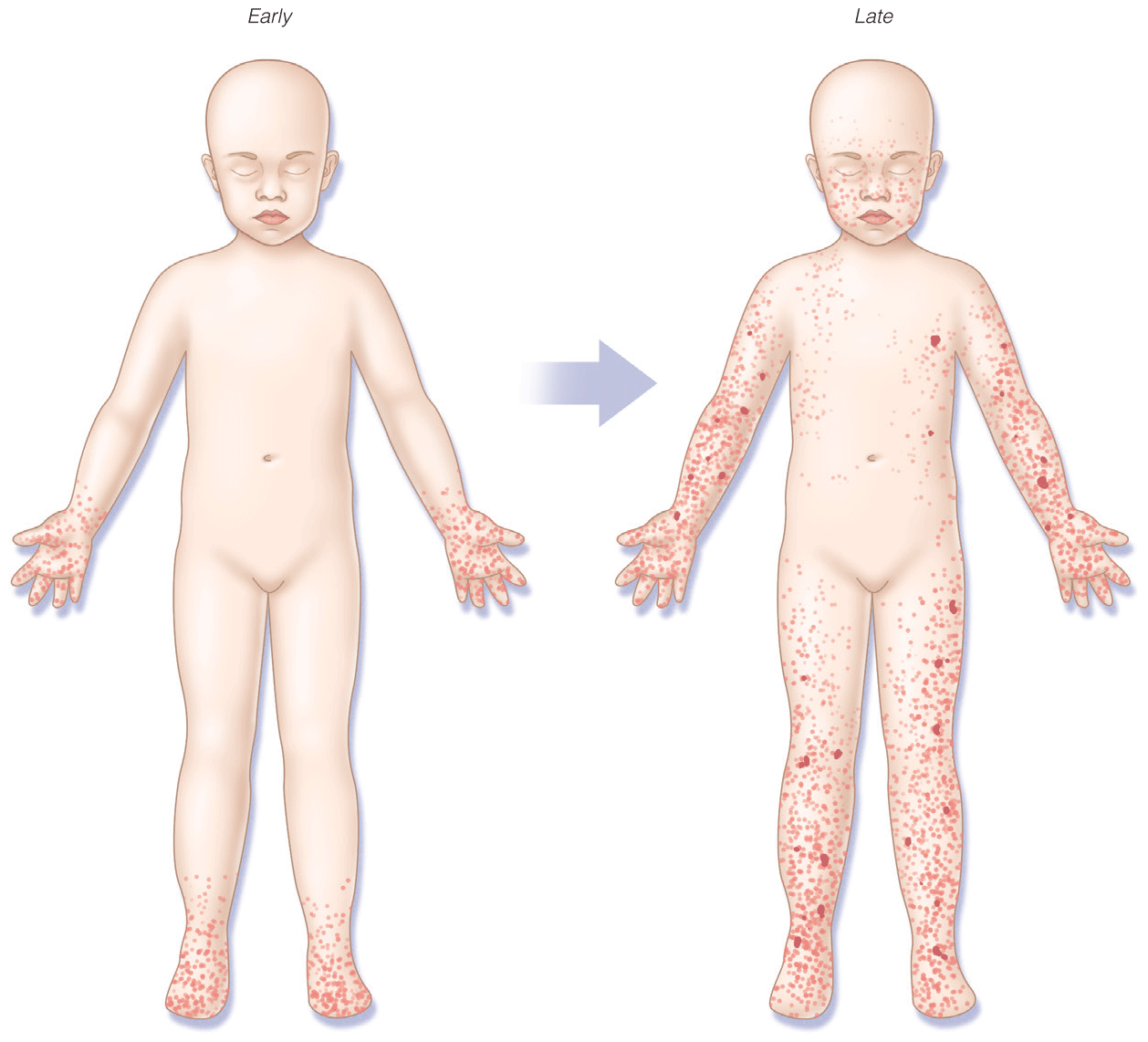
- Pediatric skin conditions are the third most common reason for presentation in the ED for children
- Suspected Rocky Mountain spotted fever should be treated immediately, before laboratory confirmation, as untreated cases can progress to serious illness or death
- Clinical scoring systems for necrotizing fasciitis and toxic epidermal necrolysis

- Pediatric skin conditions are the third most common reason for presentation in the ED for children
- Suspected Rocky Mountain spotted fever should be treated immediately, before laboratory confirmation, as untreated cases can progress to serious illness or death
- Clinical scoring systems for necrotizing fasciitis and toxic epidermal necrolysis


Pregnancy of Unknown Location and Ectopic Pregnancy
- hCG curves have been redefined to help identify abnormal pregnancies, whether in location or viability, and to further broaden the hCG values of a potentially normal pregnancy so as not to inadvertently interrupt a potentially viable pregnancy.
- Risks and benefits of single, two-dose, and multidose methotrexate therapy for medical management of ectopic pregnancy have been studied further and defined.
- Diagnostic accuracy for nontubal ectopic pregnancies is improving, but recommendations regarding treatment options remain controversial.
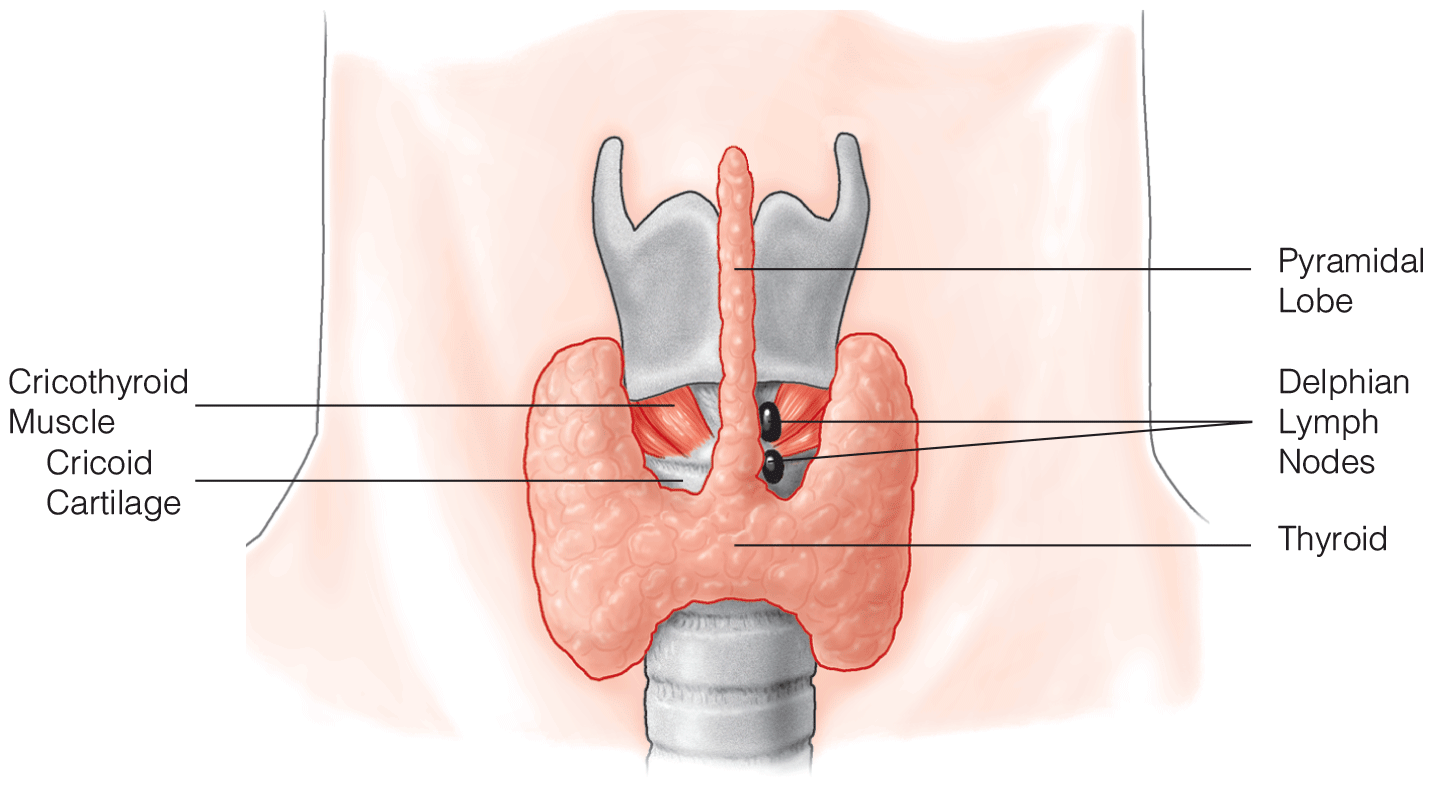
- The eighth edition of the AJCC TNM staging system has presented new stage groups for thyroid cancer subtypes.
- Intraoperative nerve monitoring is a technique that helps prevent recurrent laryngeal nerve injury during thyroidectomy.
- Minimallyinvasive video-assisted thyroidectomy and minimally invasive nonendoscopic thyroidectomy are new techniques that can be performed with or without gas insufflation; patient perceptions of cosmesis are often improved by the smaller incisions used.

- The eighth edition of the AJCC TNM staging system has presented new stage groups for thyroid cancer subtypes.
- Intraoperative nerve monitoring is a technique that helps prevent recurrent laryngeal nerve injury during thyroidectomy.
- Minimallyinvasive video-assisted thyroidectomy and minimally invasive nonendoscopic thyroidectomy are new techniques that can be performed with or without gas insufflation; patient perceptions of cosmesis are often improved by the smaller incisions used.


Postherpetic Neuralgia: A Patient’s and a Physician’s Perspective
- Today, most experts in interventional pain management recommend an evidence-based stepladder approach for the management of all patients with PHN that includes an advancing combination of therapeutic strategies as needed on a graduated basis to control pain and anxiety and prevent complications, including suicide.
- The most important immunologic risk factor for herpes zoster and PHN is the decline in cell-mediated immunity to VZV that occurs over time as people age, with an onset around 50 years of age. Although possible, second episodes of zoster are uncommon due to the boosting or anamnestic effect of the first episode of zoster.
- The nonpharmacologic treatment options for PHN include combinations of acupuncture, cryotherapy, heat therapy, and transcutaneous and/or percutaneous electrical nerve stimulation. The multimodal nonpharmacologic treatment options for PHN are stratified and compared by their evidence levels.








.png)
















