
Plastic Surgery Considerations for the General Surgeon
- Refinements of component separation have solved many problems. Rather than simply performing a suture approximation of the rectus muscles in the midline, both prosthetic and bioprosthetic meshes have been used to reinforce the midline closure as a direct supported repair.
- Skin grafts are harvested using a mechanical dermatome for split-thickness grafts or from well-hidden area of lax skin (groin crease, postauricular area) for a full-thickness graft. Skin grafts survive the transfer process from the donor to the recipient site through plasma imbibition and inosculation.
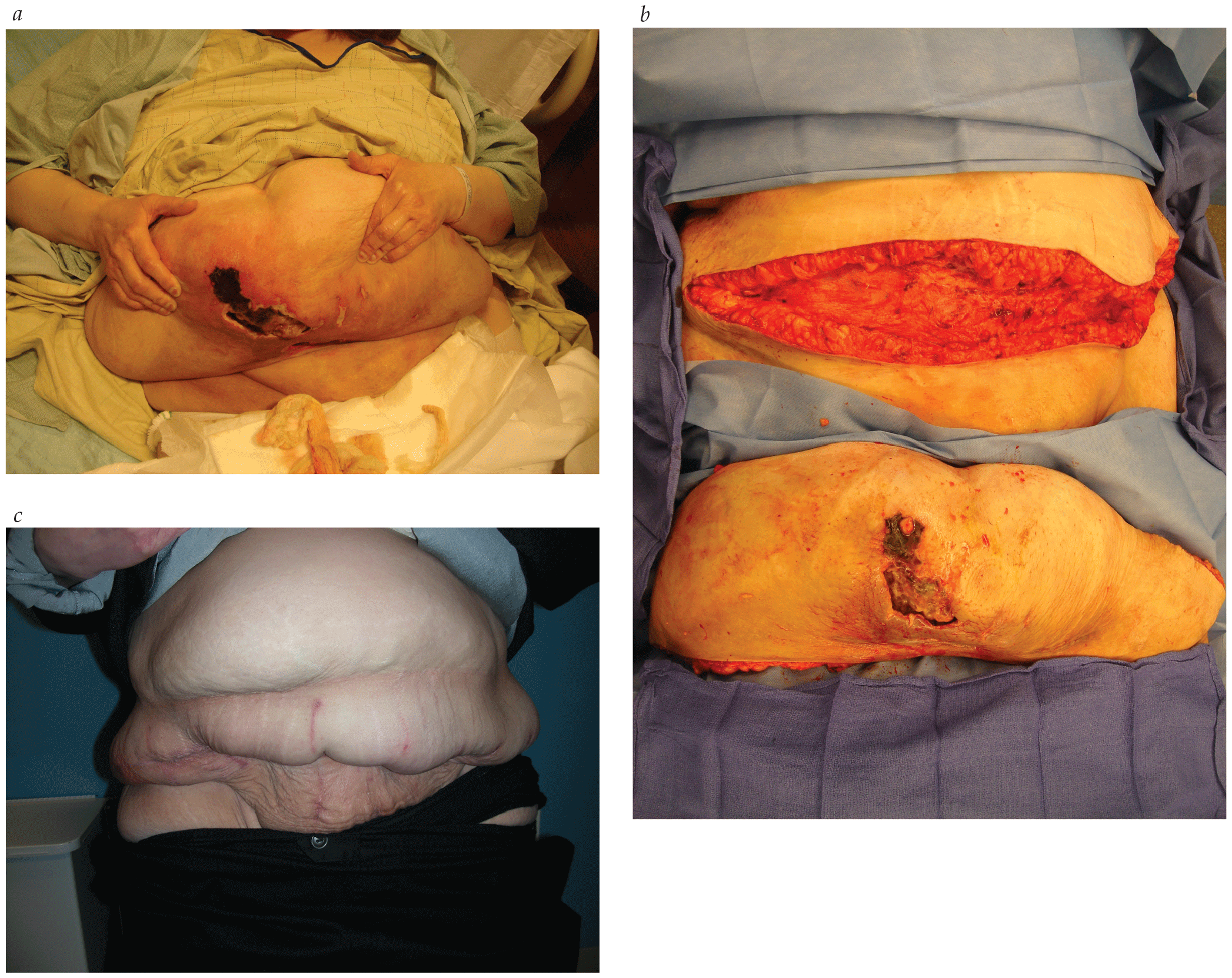
- Although many surgeons will attest to the improved exposure and access following the panniculectomy portion of the procedure, there are no randomized prospective data demonstrating improved outcomes with panniculectomy for abdominal wall access.














.png)
















