- National organizations such as the Trauma Quality Improvement Program of the American College of Surgeons have described the importance of palliative care integrated throughout the clinical course.
- Increasing numbers of surgeons are fellowship trained and certified by the American Board of Surgery in Hospice and Palliative Medicine in addition to surgical specialties.
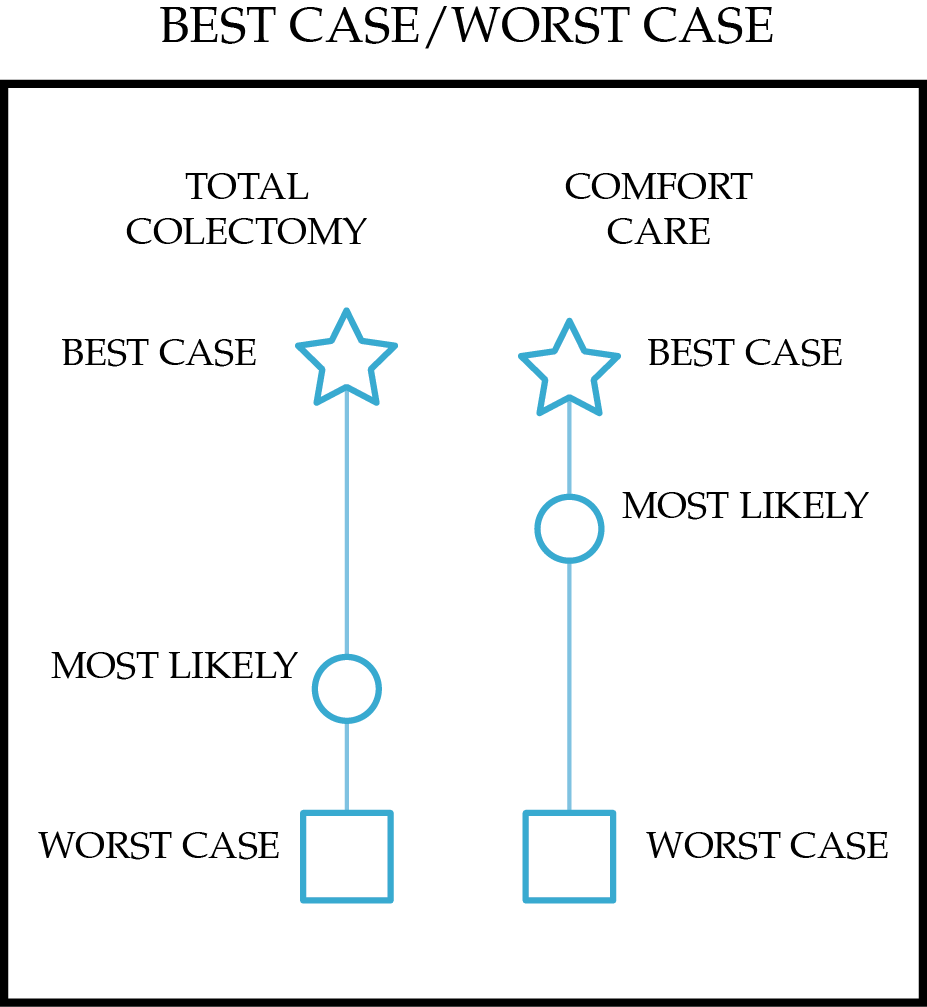
- The importance of accurate prognostication for surgical patients and thoughtful communication of anticipated outcomes of different treatment plans has been recognized through frameworks such as the “Best Case/Worst Case” scenario.1
- Structured descriptions of gaps and opportunities in the field promote future advancement and development of surgical palliative care.
- Studies in surgical and nonsurgical patients demonstrate that palliative care, hospice enrollment, and lower-intensity end-of-life care do not decrease survival.
Latest Updates


- National organizations such as the Trauma Quality Improvement Program of the American College of Surgeons have described the importance of palliative care integrated throughout the clinical course.
- Increasing numbers of surgeons are fellowship trained and certified by the American Board of Surgery in Hospice and Palliative Medicine in addition to surgical specialties.
- The importance of accurate prognostication for surgical patients and thoughtful communication of anticipated outcomes of different treatment plans has been recognized through frameworks such as the “Best Case/Worst Case” scenario.1
- Structured descriptions of gaps and opportunities in the field promote future advancement and development of surgical palliative care.
- Studies in surgical and nonsurgical patients demonstrate that palliative care, hospice enrollment, and lower-intensity end-of-life care do not decrease survival.

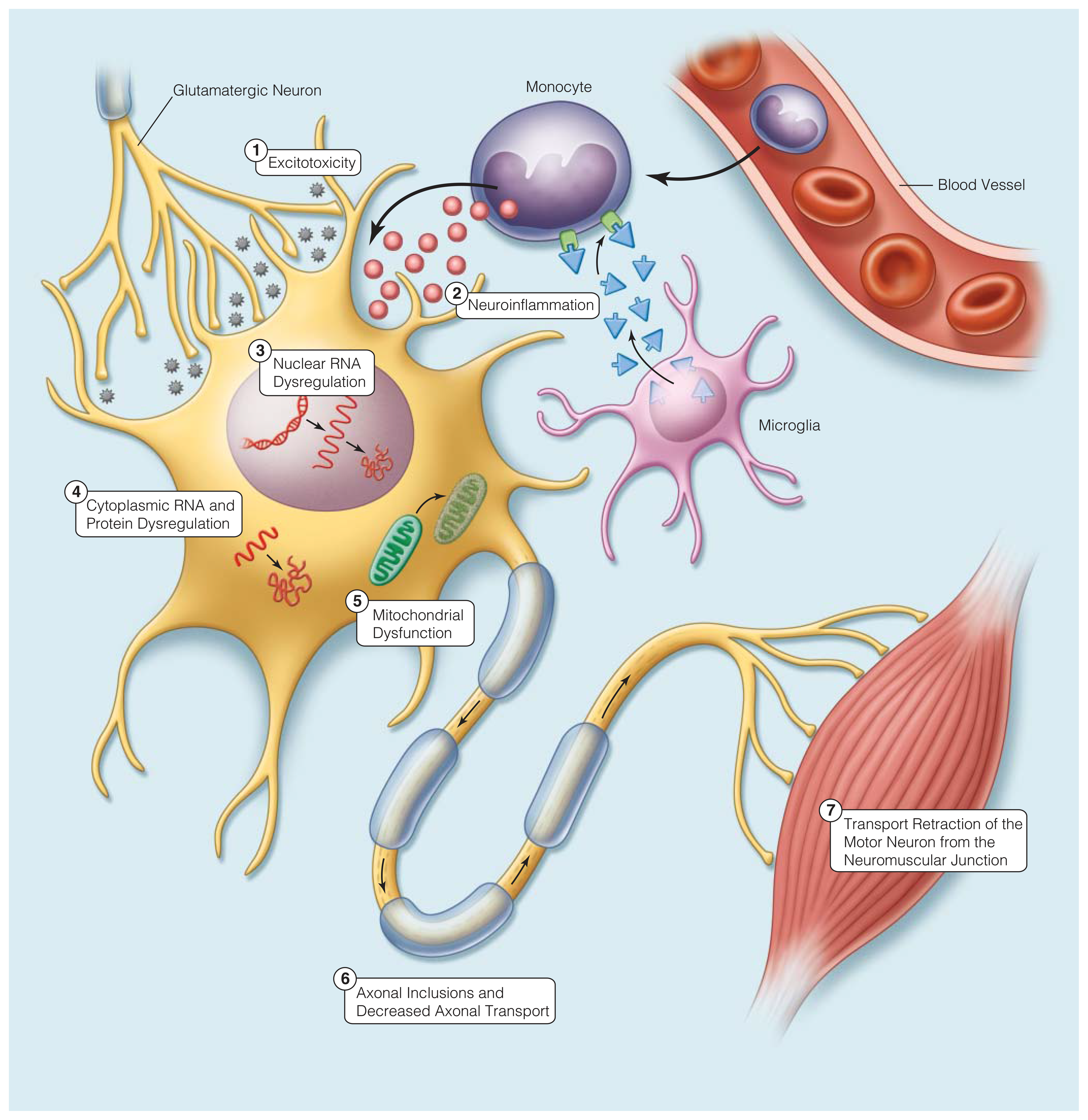
- The genetic advances of the early 1990s and the subsequent development of disease models have propelled the field forward. Since then, there has been an exponentially increasing rate of genes discovered to be associated with ALS. More than 25 genetic abnormalities have been identified to cause disease, some of which have also been implicated in PLS and PMA.
- Because only a small proportion of ALS is familial, and because the commercially available gene testing covers only a portion of the causative genes for ALS, genetic testing cannot be used to exclude a diagnosis of ALS. However, patients with a family history of ALS should receive genetic counseling and be offered genetic testing to identify a causative mutation.
- There is an ongoing effort to uncover markers of disease in the blood, CSF, urine, or other body fluid in patients with ALS. The discovery of a diagnostic biomarker for ALS could reduce diagnostic delay, and a biomarker of disease progression could serve as an outcome for trials.

- National organizations such as the Trauma Quality Improvement Program of the American College of Surgeons have described the importance of palliative care integrated throughout the clinical course.
- Increasing numbers of surgeons are fellowship trained and certified by the American Board of Surgery in Hospice and Palliative Medicine in addition to surgical specialties.
- The importance of accurate prognostication for surgical patients and thoughtful communication of anticipated outcomes of different treatment plans has been recognized through frameworks such as the “Best Case/Worst Case” scenario.1
- Structured descriptions of gaps and opportunities in the field promote future advancement and development of surgical palliative care.
- Studies in surgical and nonsurgical patients demonstrate that palliative care, hospice enrollment, and lower-intensity end-of-life care do not decrease survival.

- The genetic advances of the early 1990s and the subsequent development of disease models have propelled the field forward. Since then, there has been an exponentially increasing rate of genes discovered to be associated with ALS. More than 25 genetic abnormalities have been identified to cause disease, some of which have also been implicated in PLS and PMA.
- Because only a small proportion of ALS is familial, and because the commercially available gene testing covers only a portion of the causative genes for ALS, genetic testing cannot be used to exclude a diagnosis of ALS. However, patients with a family history of ALS should receive genetic counseling and be offered genetic testing to identify a causative mutation.
- There is an ongoing effort to uncover markers of disease in the blood, CSF, urine, or other body fluid in patients with ALS. The discovery of a diagnostic biomarker for ALS could reduce diagnostic delay, and a biomarker of disease progression could serve as an outcome for trials.

- National organizations such as the Trauma Quality Improvement Program of the American College of Surgeons have described the importance of palliative care integrated throughout the clinical course.
- Increasing numbers of surgeons are fellowship trained and certified by the American Board of Surgery in Hospice and Palliative Medicine in addition to surgical specialties.
- The importance of accurate prognostication for surgical patients and thoughtful communication of anticipated outcomes of different treatment plans has been recognized through frameworks such as the “Best Case/Worst Case” scenario.1
- Structured descriptions of gaps and opportunities in the field promote future advancement and development of surgical palliative care.
- Studies in surgical and nonsurgical patients demonstrate that palliative care, hospice enrollment, and lower-intensity end-of-life care do not decrease survival.

- The genetic advances of the early 1990s and the subsequent development of disease models have propelled the field forward. Since then, there has been an exponentially increasing rate of genes discovered to be associated with ALS. More than 25 genetic abnormalities have been identified to cause disease, some of which have also been implicated in PLS and PMA.
- Because only a small proportion of ALS is familial, and because the commercially available gene testing covers only a portion of the causative genes for ALS, genetic testing cannot be used to exclude a diagnosis of ALS. However, patients with a family history of ALS should receive genetic counseling and be offered genetic testing to identify a causative mutation.
- There is an ongoing effort to uncover markers of disease in the blood, CSF, urine, or other body fluid in patients with ALS. The discovery of a diagnostic biomarker for ALS could reduce diagnostic delay, and a biomarker of disease progression could serve as an outcome for trials.

- The genetic advances of the early 1990s and the subsequent development of disease models have propelled the field forward. Since then, there has been an exponentially increasing rate of genes discovered to be associated with ALS. More than 25 genetic abnormalities have been identified to cause disease, some of which have also been implicated in PLS and PMA.
- Because only a small proportion of ALS is familial, and because the commercially available gene testing covers only a portion of the causative genes for ALS, genetic testing cannot be used to exclude a diagnosis of ALS. However, patients with a family history of ALS should receive genetic counseling and be offered genetic testing to identify a causative mutation.
- There is an ongoing effort to uncover markers of disease in the blood, CSF, urine, or other body fluid in patients with ALS. The discovery of a diagnostic biomarker for ALS could reduce diagnostic delay, and a biomarker of disease progression could serve as an outcome for trials.







.png)
















