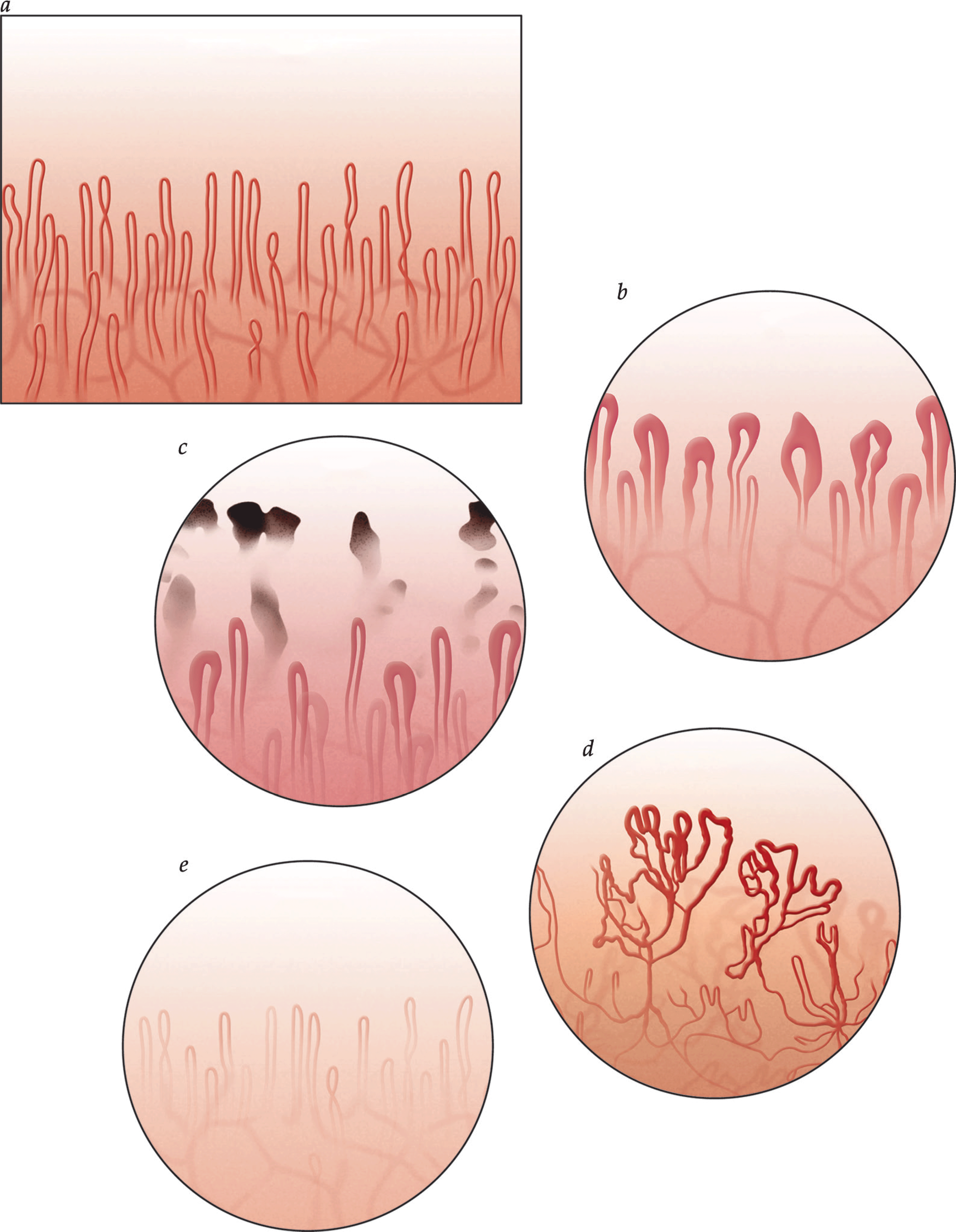
- Raynaud phenomenon has two forms: primary and secondary based on the presence or absence of associated disease processes.
- Raynaud phenomenon is an exaggerated vasospastic response to stimuli that results in digital discoloration.
- Environmental modification is the initial therapy.
- Pharmacologic treatment is most commonly used when environmental modification fails.
- Injections and surgery are sometimes necessary in severe, resistant forms of the disease process.
Latest Updates



Cutaneous Adverse Drug Reactions
- The treatment of simple exanthematous eruptions is generally supportive. For example, oral antihistamines used in conjunction with soothing baths may help relieve pruritus. Topical corticosteroids are indicated when antihistamines do not provide relief. Systemic corticosteroids are used only in severe cases. Discontinuance of the offending agent is recommended in most cases.
- Sulfonamide antibiotics can cause hypersensitivity syndrome reactions in susceptible persons. The primary metabolic pathway for sulfonamides involves acetylation of the drug to a nontoxic metabolite and renal excretion. An alternative metabolic pathway, quantitatively more important in patients who are slow acetylators, engages the cytochrome P-450 mixed-function oxidase system.
- Differentiation within the spectrum of SJS and TEN depends on the nature of the skin lesions and extent of body surface area involvement. Clinically, reactions of SJS/TEN spectrum are characterized by the presence of the triad of mucous membrane erosions, target lesions, and epidermal necrosis with skin detachment.62 Detachment of less than 10% of the total body surface area is part of the definition of SJS, whereas TEN occurs when there is greater than 30% body surface involvement; intermediate cases have been called SJS/TEN overlap (10 to 30%).

Cutaneous Adverse Drug Reactions
- The treatment of simple exanthematous eruptions is generally supportive. For example, oral antihistamines used in conjunction with soothing baths may help relieve pruritus. Topical corticosteroids are indicated when antihistamines do not provide relief. Systemic corticosteroids are used only in severe cases. Discontinuance of the offending agent is recommended in most cases.
- Sulfonamide antibiotics can cause hypersensitivity syndrome reactions in susceptible persons. The primary metabolic pathway for sulfonamides involves acetylation of the drug to a nontoxic metabolite and renal excretion. An alternative metabolic pathway, quantitatively more important in patients who are slow acetylators, engages the cytochrome P-450 mixed-function oxidase system.
- Differentiation within the spectrum of SJS and TEN depends on the nature of the skin lesions and extent of body surface area involvement. Clinically, reactions of SJS/TEN spectrum are characterized by the presence of the triad of mucous membrane erosions, target lesions, and epidermal necrosis with skin detachment.62 Detachment of less than 10% of the total body surface area is part of the definition of SJS, whereas TEN occurs when there is greater than 30% body surface involvement; intermediate cases have been called SJS/TEN overlap (10 to 30%).

Cutaneous Adverse Drug Reactions
- The treatment of simple exanthematous eruptions is generally supportive. For example, oral antihistamines used in conjunction with soothing baths may help relieve pruritus. Topical corticosteroids are indicated when antihistamines do not provide relief. Systemic corticosteroids are used only in severe cases. Discontinuance of the offending agent is recommended in most cases.
- Sulfonamide antibiotics can cause hypersensitivity syndrome reactions in susceptible persons. The primary metabolic pathway for sulfonamides involves acetylation of the drug to a nontoxic metabolite and renal excretion. An alternative metabolic pathway, quantitatively more important in patients who are slow acetylators, engages the cytochrome P-450 mixed-function oxidase system.
- Differentiation within the spectrum of SJS and TEN depends on the nature of the skin lesions and extent of body surface area involvement. Clinically, reactions of SJS/TEN spectrum are characterized by the presence of the triad of mucous membrane erosions, target lesions, and epidermal necrosis with skin detachment.62 Detachment of less than 10% of the total body surface area is part of the definition of SJS, whereas TEN occurs when there is greater than 30% body surface involvement; intermediate cases have been called SJS/TEN overlap (10 to 30%).
Cutaneous Adverse Drug Reactions
- The treatment of simple exanthematous eruptions is generally supportive. For example, oral antihistamines used in conjunction with soothing baths may help relieve pruritus. Topical corticosteroids are indicated when antihistamines do not provide relief. Systemic corticosteroids are used only in severe cases. Discontinuance of the offending agent is recommended in most cases.
- Sulfonamide antibiotics can cause hypersensitivity syndrome reactions in susceptible persons. The primary metabolic pathway for sulfonamides involves acetylation of the drug to a nontoxic metabolite and renal excretion. An alternative metabolic pathway, quantitatively more important in patients who are slow acetylators, engages the cytochrome P-450 mixed-function oxidase system.
- Differentiation within the spectrum of SJS and TEN depends on the nature of the skin lesions and extent of body surface area involvement. Clinically, reactions of SJS/TEN spectrum are characterized by the presence of the triad of mucous membrane erosions, target lesions, and epidermal necrosis with skin detachment.62 Detachment of less than 10% of the total body surface area is part of the definition of SJS, whereas TEN occurs when there is greater than 30% body surface involvement; intermediate cases have been called SJS/TEN overlap (10 to 30%).

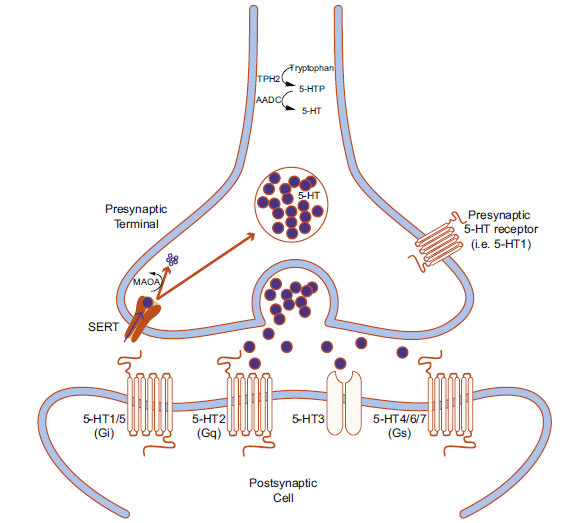
- Drug discovery targets include receptors, enzymes, and transporters.
- Serotonin, dopamine, norepinephrine, γ-aminobutyric acid, glutamate, and acetylcholine play important roles in neuropsychiatric functions and are targets for many FDA-approved psychiatric medications.
- Understanding the basics of neurotransmission, enzyme degradation, and receptor and transporter pharmacology is essential to understand psychiatric medications.
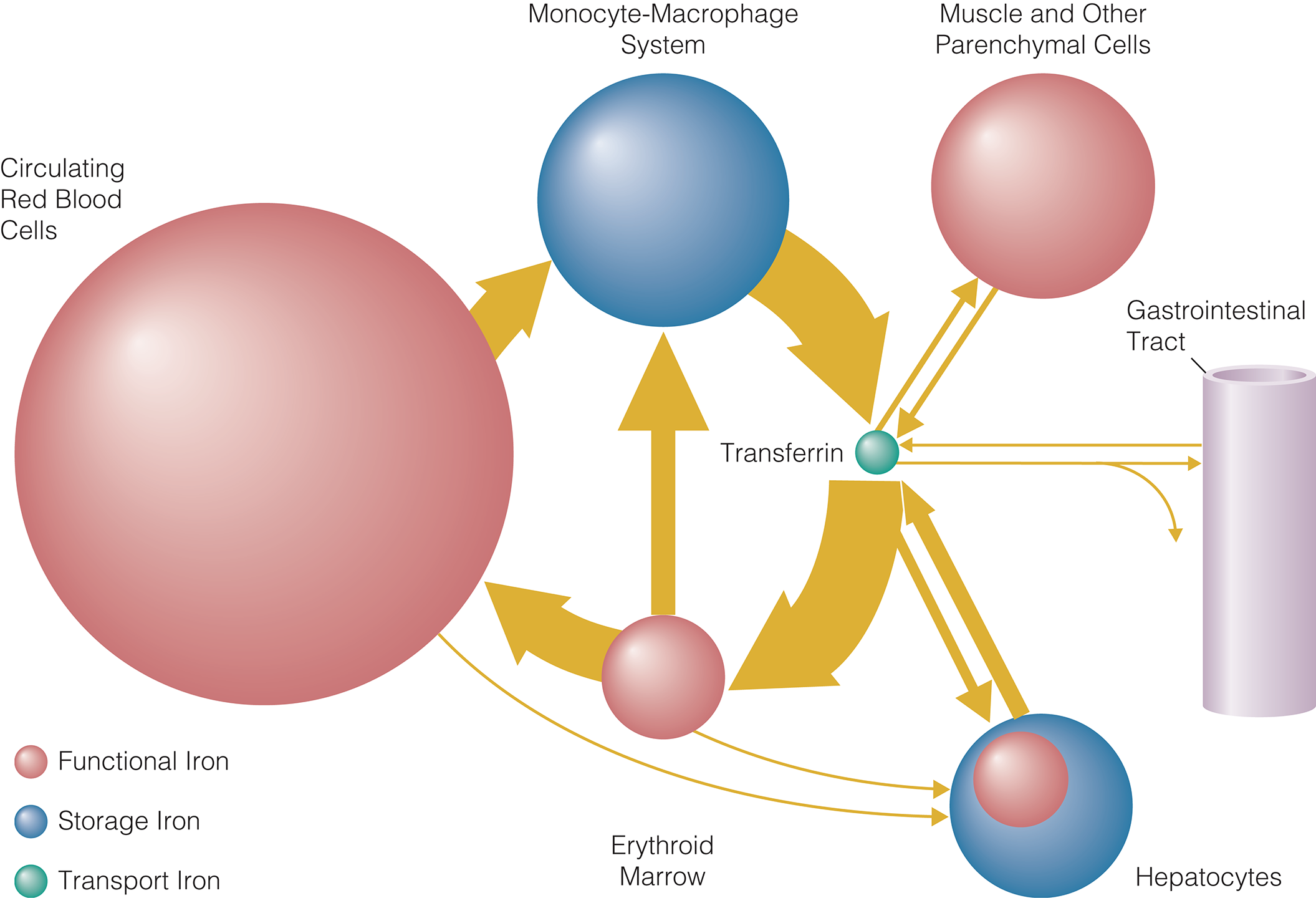
Red Blood Cell Function and Disorders of Iron Metabolism
- Iron deficiency should be understood as a stage in the spectrum of negative iron balance. Negative iron balance exists when the body’s iron requirements exceed iron supply. Iron is needed to restore basal physiologic loss from exfoliated skin or mucosal cells, which is approximately 14 µg/kg/day.
- For blood donors, each donation results in the loss of 200 to 250 mg of iron.33 During periods of growth in infancy, childhood, and adolescence, iron requirements may outstrip the supply of iron available from diet and stores. In addition, children fed whole cow’s milk may develop gastrointestinal bleeding, leading to iron deficiency.
- A decreased serum ferritin concentration is the most specific indicator of iron deficiency. A serum ferritin concentration below 15 to 20 µg/L is diagnostic of absent or nearly absent iron stores, regardless of the laboratory methodology used. In contrast, a normal serum ferritin concentration does not confirm the presence of storage iron because serum ferritin concentration may be increased independently of body iron by infection, inflammation, liver disease, malignancy, and other conditions.
Red Blood Cell Function and Disorders of Iron Metabolism
- Iron deficiency should be understood as a stage in the spectrum of negative iron balance. Negative iron balance exists when the body’s iron requirements exceed iron supply. Iron is needed to restore basal physiologic loss from exfoliated skin or mucosal cells, which is approximately 14 µg/kg/day.
- For blood donors, each donation results in the loss of 200 to 250 mg of iron.33 During periods of growth in infancy, childhood, and adolescence, iron requirements may outstrip the supply of iron available from diet and stores. In addition, children fed whole cow’s milk may develop gastrointestinal bleeding, leading to iron deficiency.
- A decreased serum ferritin concentration is the most specific indicator of iron deficiency. A serum ferritin concentration below 15 to 20 µg/L is diagnostic of absent or nearly absent iron stores, regardless of the laboratory methodology used. In contrast, a normal serum ferritin concentration does not confirm the presence of storage iron because serum ferritin concentration may be increased independently of body iron by infection, inflammation, liver disease, malignancy, and other conditions.








.png)


















