Evaluation and Management of Cleft Lip and Palate
- Lip Taping and nasoalveolar molding pre-operatively can greatly improve surgical outcomes.
- 3-Dimensional printing used to make nasoalveolar molding appliances

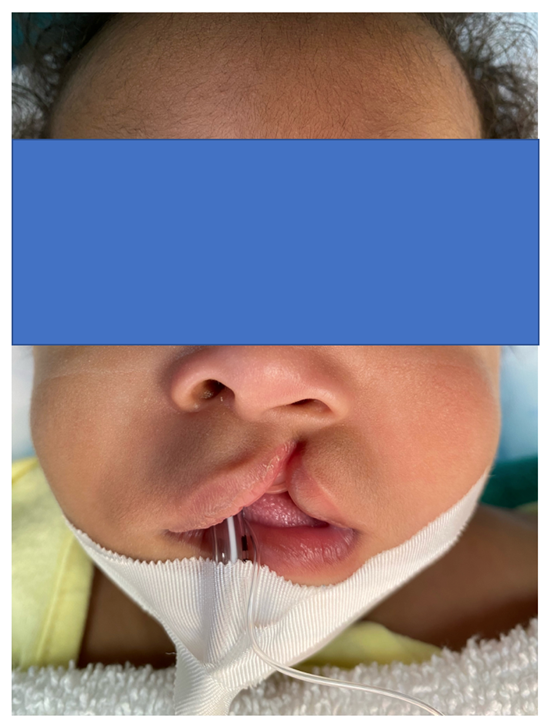
Evaluation and Management of Cleft Lip and Palate

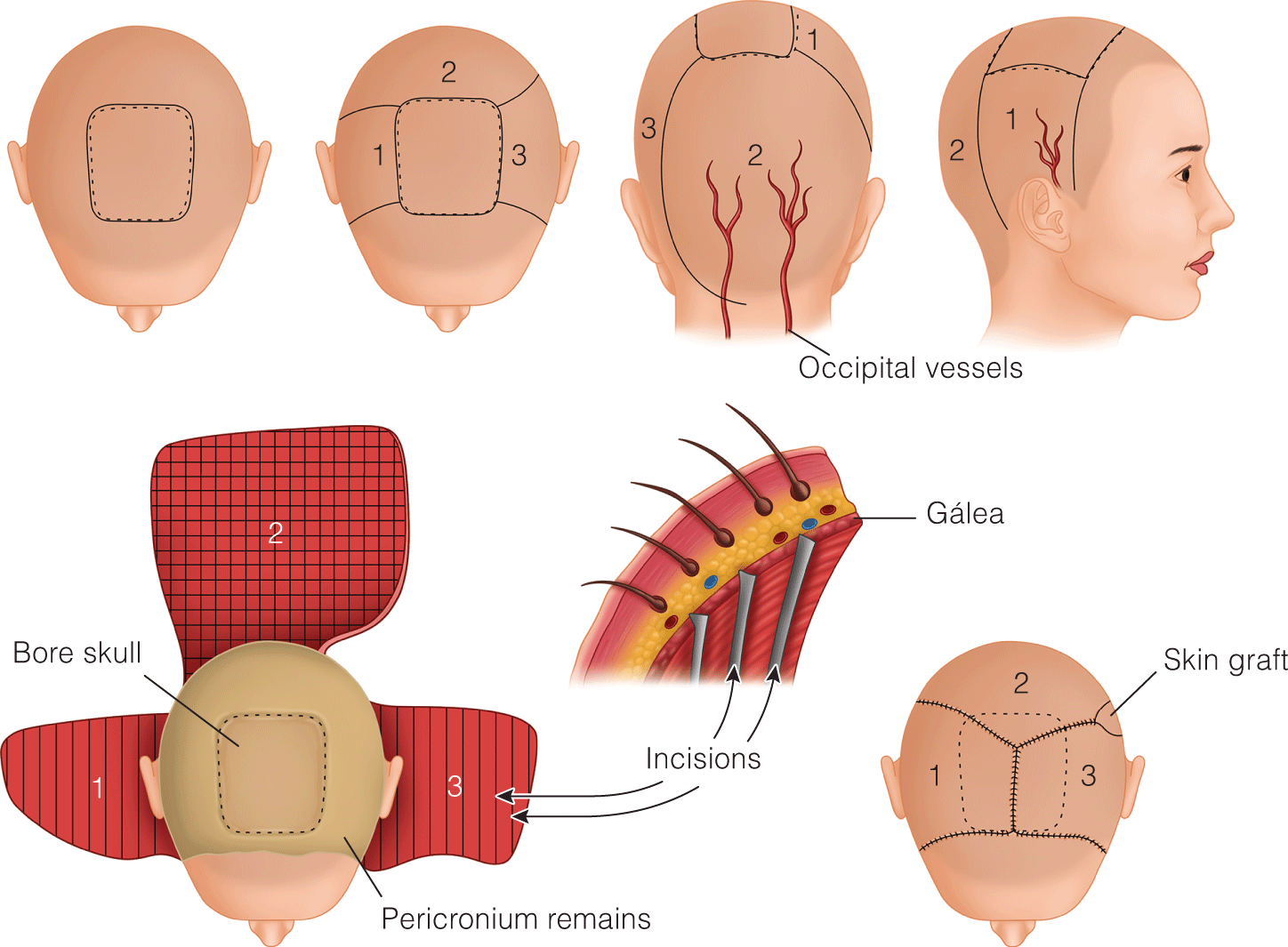
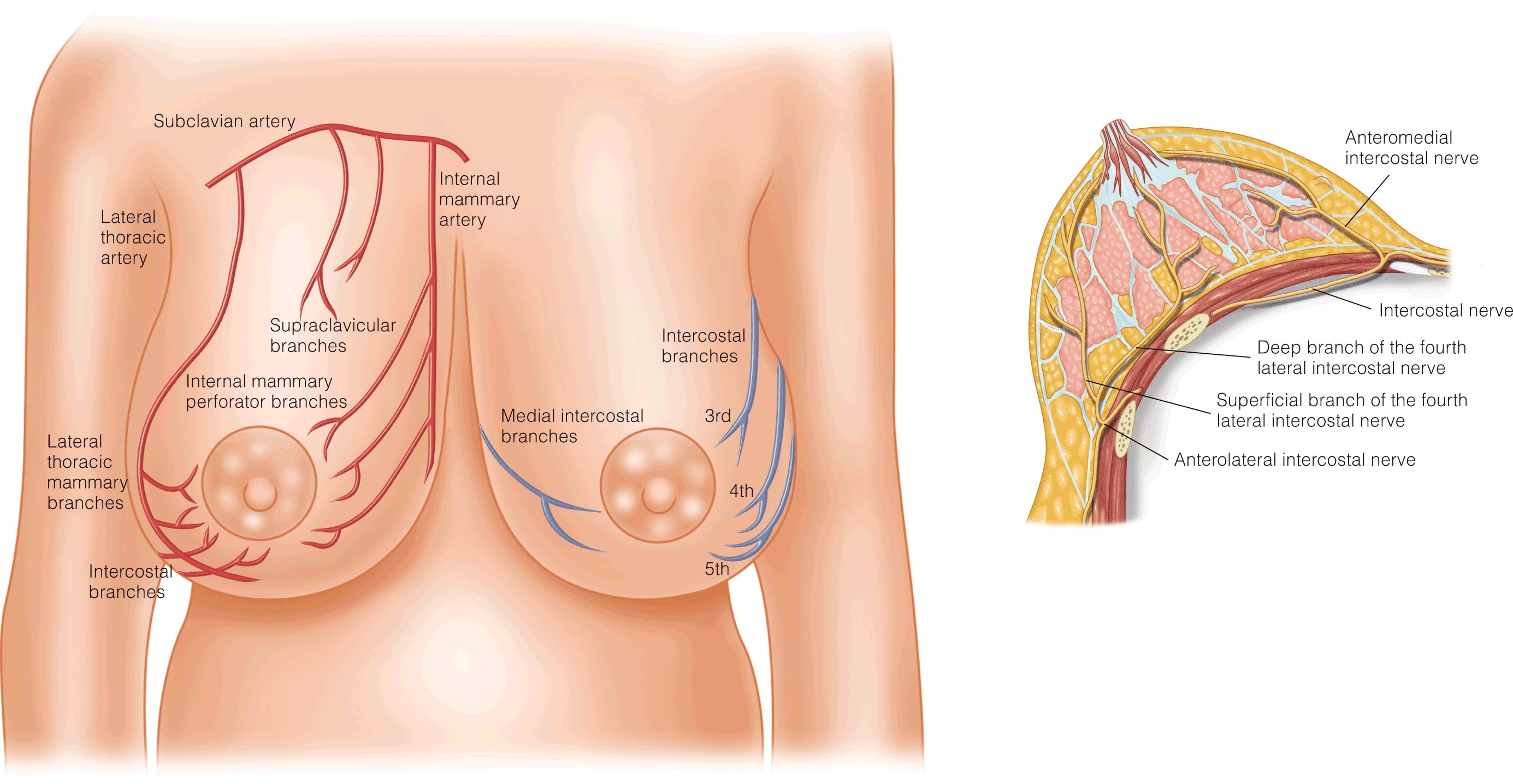
Lip, Cheek, & Scalp Reconstruction

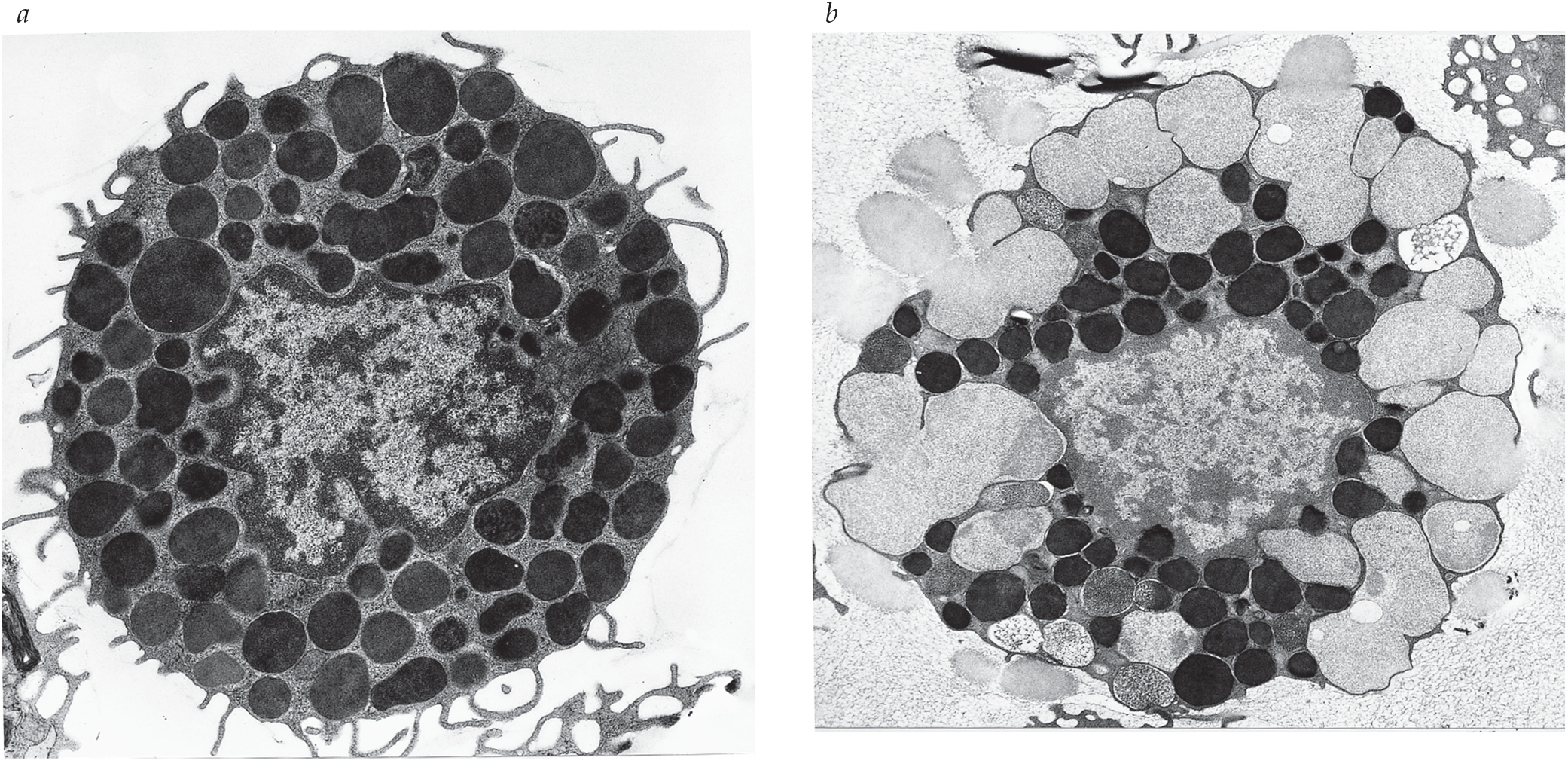
Allergic Response

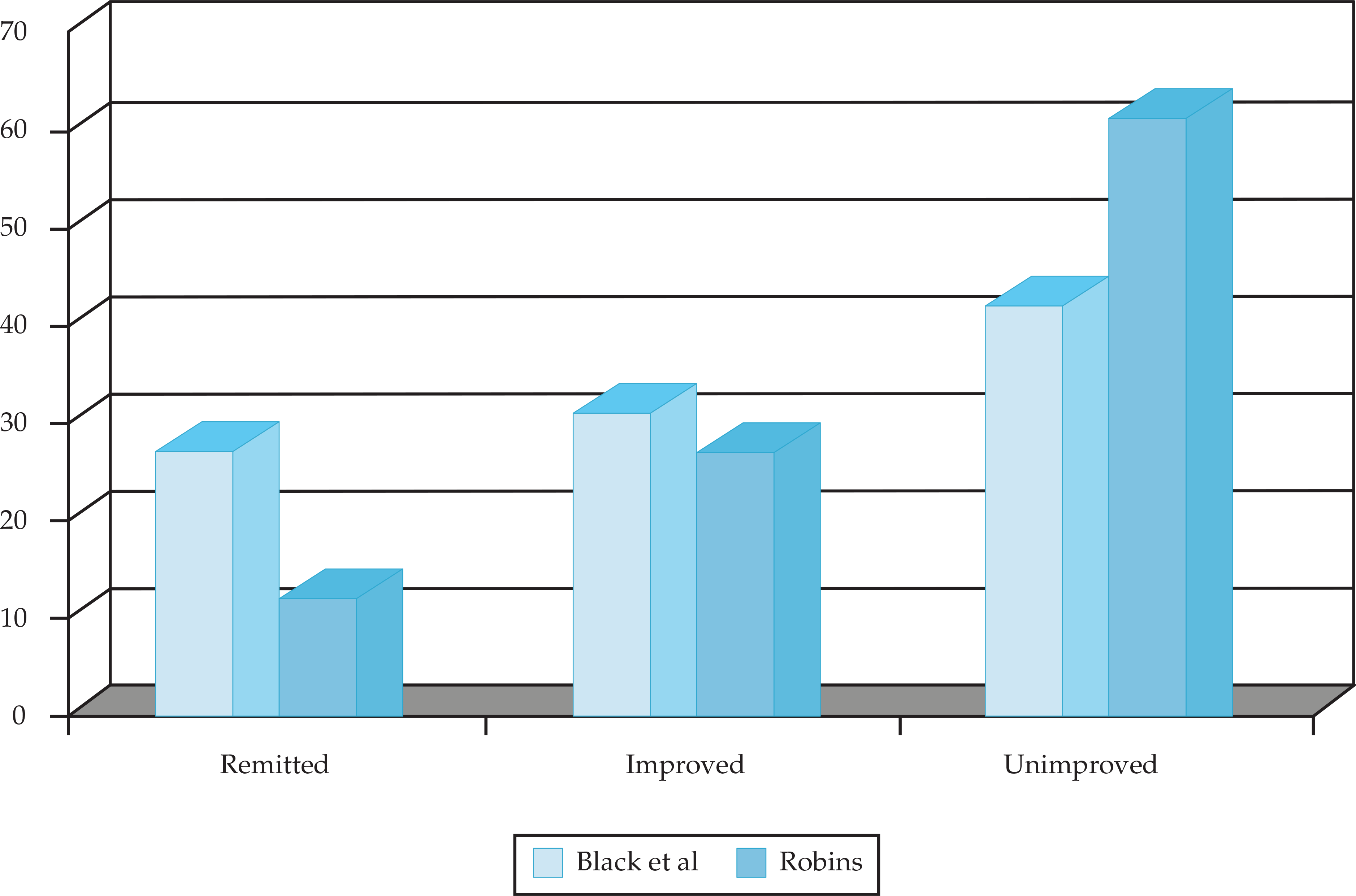
Antisocial Personality Disorder and Its Clinical Management

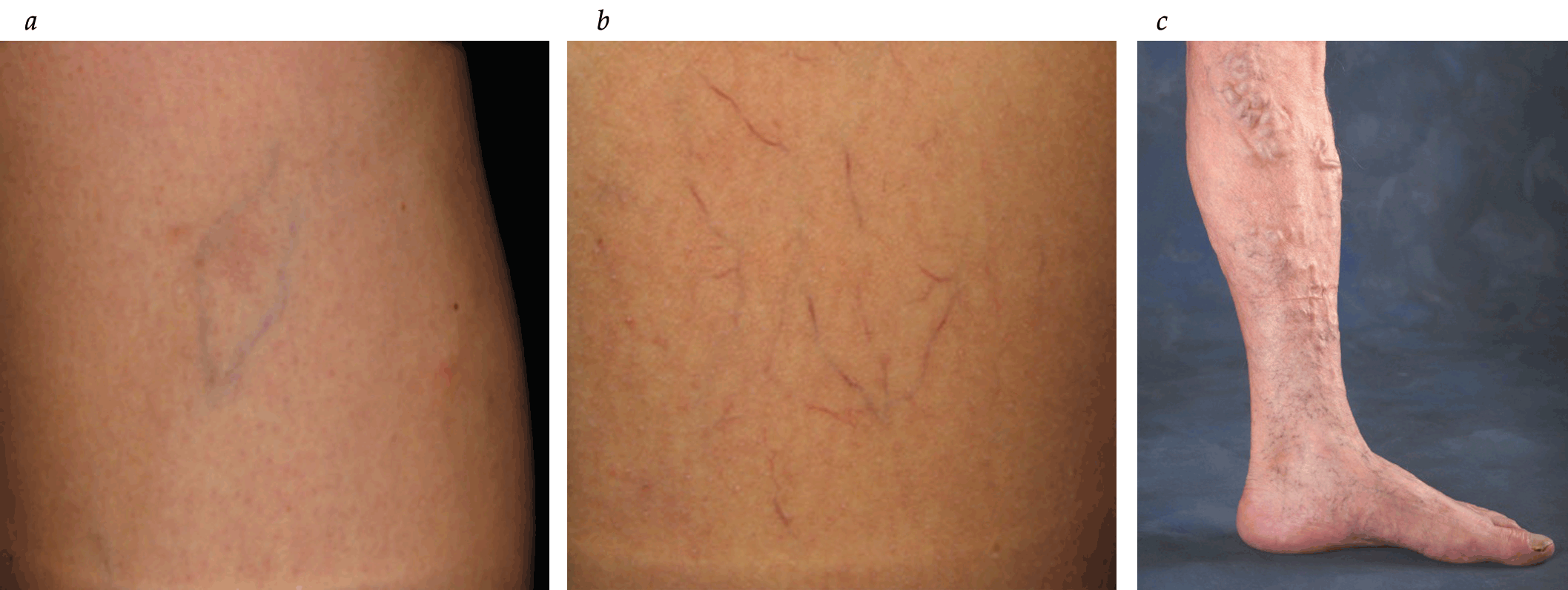
Injection Sclerotherapy and Ablation


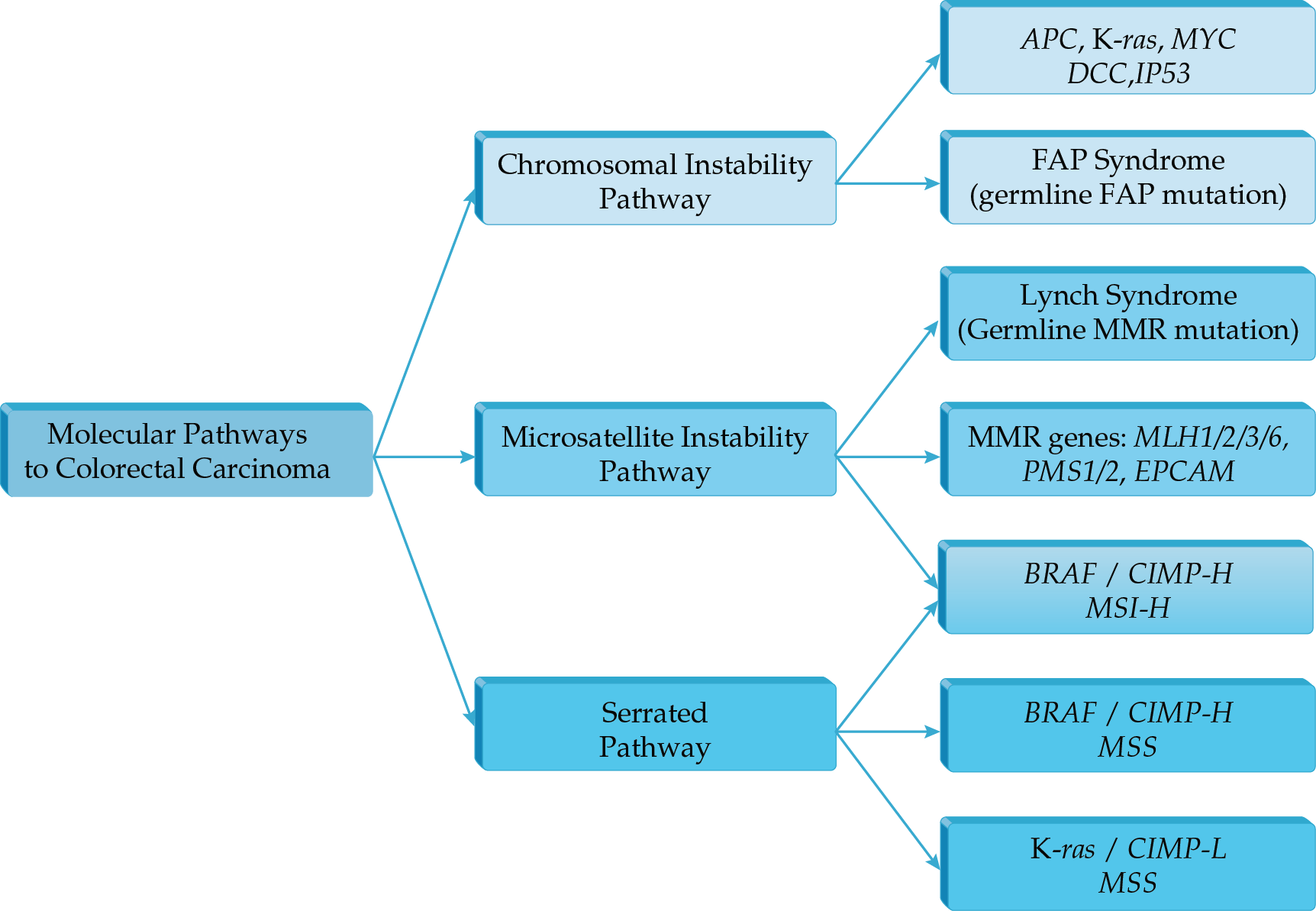
Epidemiology and Molecular Biology of Colorectal Cancer
Customize by choosing your prefered medical database







.png)

















