- Subdural hematoma and traumatic subarachnoid blood are the most common hemorrhagic computed tomographic (CT) findings in patients with head injury.
- In the patient with signs of brain herniation and borderline or shock vital signs, the ideal hyperosmotic agent is hypertonic saline.
- Although the incidence of traumatic findings on a cranial CT scan in patients with head injury, loss of consciousness, and a Glasgow Coma Scale score of 15 is about 6%, the need for neurosurgical intervention in this cohort is 0.4%.
- Guidelines for ordering CT scans in adults after head trauma are the Canadian CT head rule and the New Orleans criteria. The guideline for pediatric patients is the PECARN set of rules.
- Four-factor prothrombin complex concentrate can rapidly reverse the effects of warfarin in patients with intracranial hemorrhage.
- For the athlete with head injury, immediate removal from play and a graded increase in activity as long as the patient is asymptomatic are the basis of concussion management.
Latest Updates



- Subdural hematoma and traumatic subarachnoid blood are the most common hemorrhagic computed tomographic (CT) findings in patients with head injury.
- In the patient with signs of brain herniation and borderline or shock vital signs, the ideal hyperosmotic agent is hypertonic saline.
- Although the incidence of traumatic findings on a cranial CT scan in patients with head injury, loss of consciousness, and a Glasgow Coma Scale score of 15 is about 6%, the need for neurosurgical intervention in this cohort is 0.4%.
- Guidelines for ordering CT scans in adults after head trauma are the Canadian CT head rule and the New Orleans criteria. The guideline for pediatric patients is the PECARN set of rules.
- Four-factor prothrombin complex concentrate can rapidly reverse the effects of warfarin in patients with intracranial hemorrhage.
- For the athlete with head injury, immediate removal from play and a graded increase in activity as long as the patient is asymptomatic are the basis of concussion management.
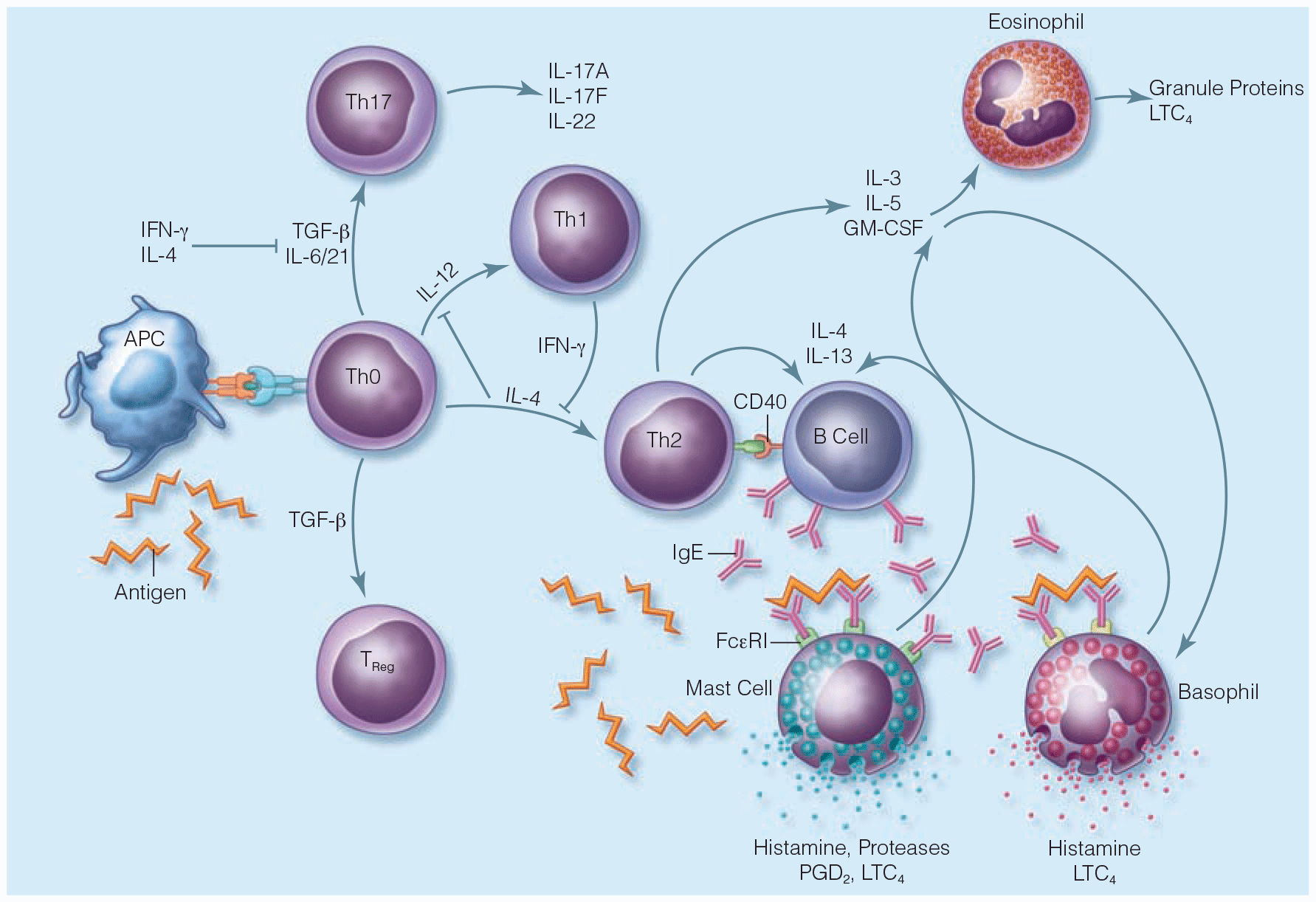
Hypersensitivity Reactions and Anaphylaxis
- Novel therapies with the potential for management of anaphylaxis are currently being investigated. Omalizumab, a monoclonal antibody, has several proposed mechanisms of action, among which includes the rapid reduction of the level of free immunoglobulin E (IgE) in serum. Omalizumab has been approved and used in the treatment of patients with moderate to severe asthma as well as other IgE-mediated allergic disorders. Although there have been case reports regarding its use in anaphylaxis, ongoing research is needs to be performed.
- Another potential therapy for anaphylaxis is methylene blue. It has been show to inhibit the relaxation of smooth muscle in vessels that lead to vasodilation and shock. Animal studies have demonstrated the potential of methylene blue in the prevention of cerebral ischemia associated with anaphylactic shock; however, more research is needed.
.png)
- ATS guidelines for exercise-induced bronchoconstriction, asthma in the elderly, and asthma in the workplace
- ERS/ATS guideline for severe asthma discusses pharmacologic modalities of asthma management and bronchial thermoplasty.
- 2020 GINA practice guidelines no longer recommend treatment with SABA alone, without inhaled ICS. Recommend that all adults and adolescents with asthma should receive ICS-containing controller treatment.
- 2020 NAEPP practice guidelines delineating optimal treatment steps in adolescents and adults with asthma. This includes bronchial thermoplasty and immunotherapy.
Unstable Angina and Non-ST Segment Elevation Acute Coronary Syndrome
- Beta blockers remain underused in clinical practice despite demonstrated efficacy in acute myocardial infarction (AMI). They have been shown to reduce myocardial oxygen demand and infarction size, and alleviate AMI-related pain. They also reduce the likelihood of developing mechanical and arrhythmogenic complications of AMI. They can be dosed in a wide range, and should be started at the lower end of the dosing range and titrated upward. The only relative contraindications to treatment with beta blockers are mild to moderate heart failure, obstructive airway disease (in the absence of asthma), peripheral vascular disease, diabetes mellitus and a history of cardiomyopathy.
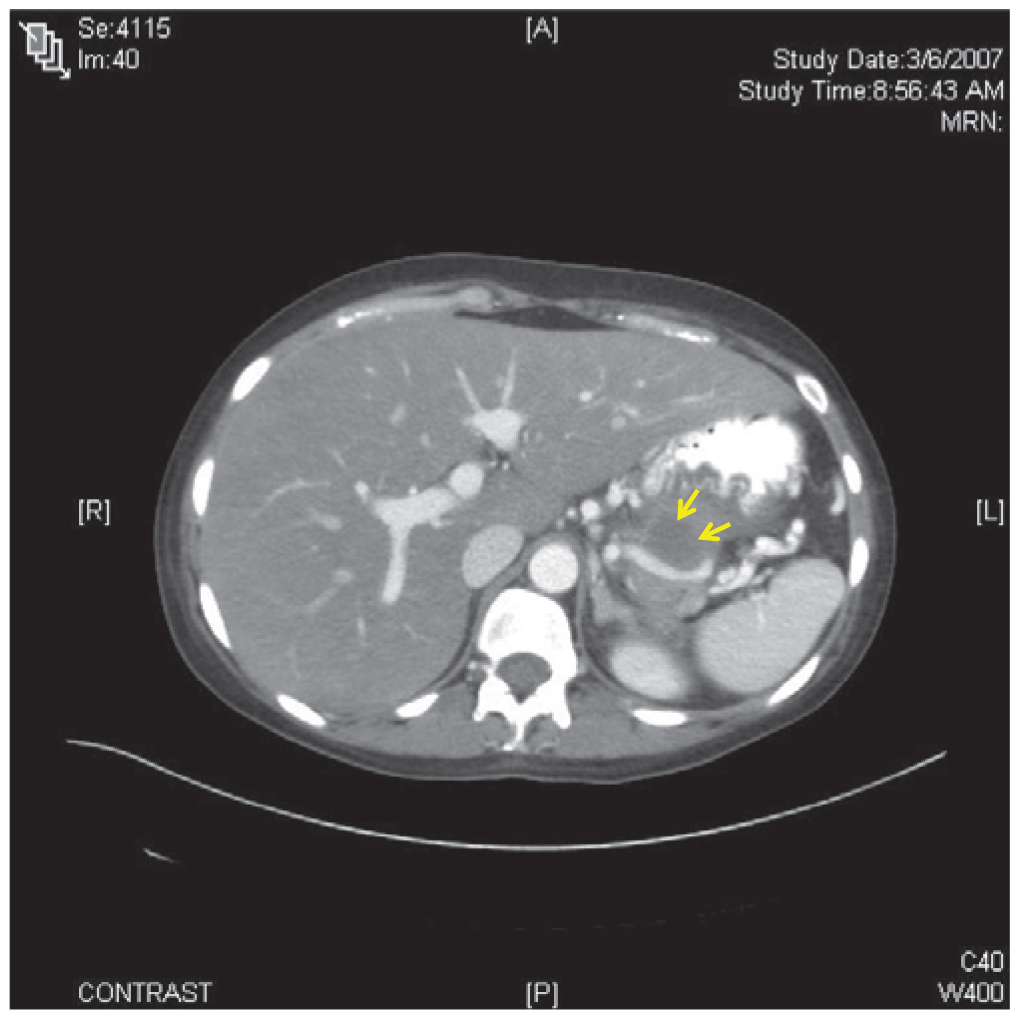
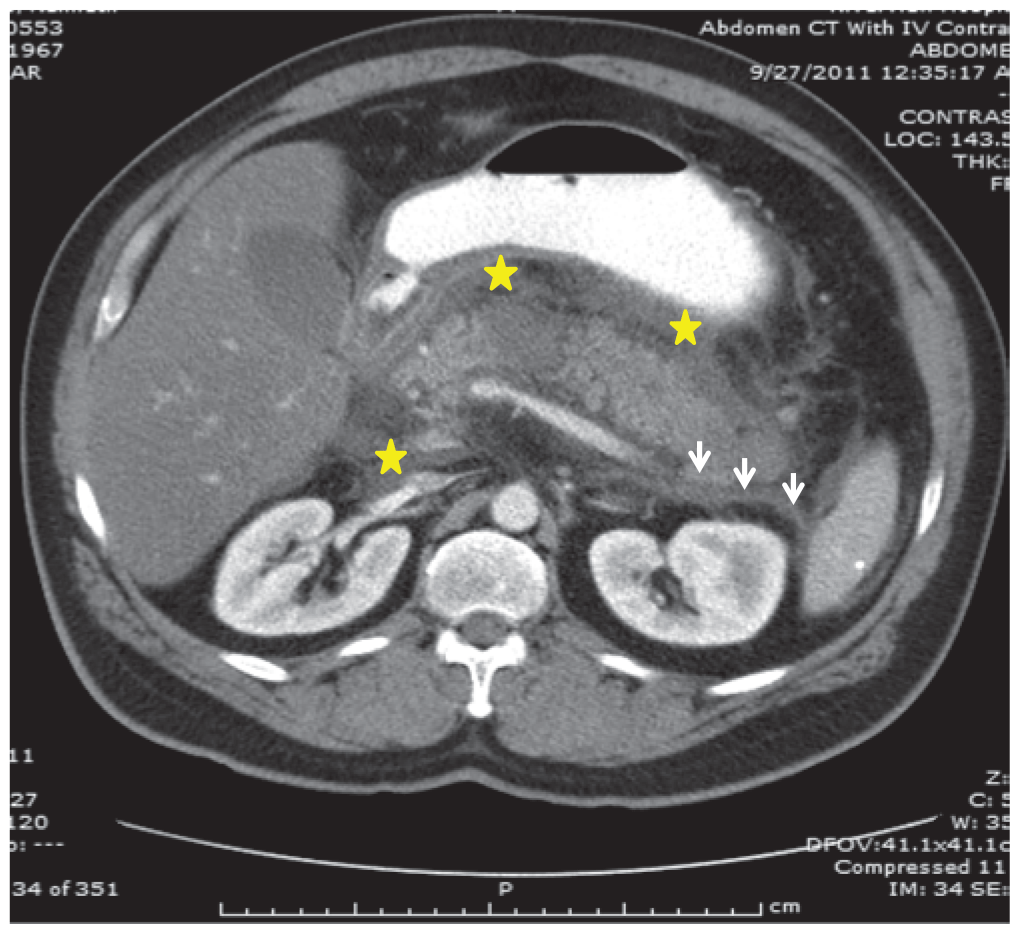
- The chief presenting complaint in acute pancreatitis is abdominal pain. The differential diagnosis for pancreatitis is broad, and includes abdominal, pulmonary, urologic and cardiovascular pathologies.
- Recent guidelines state that the diagnosis of acute pancreatitis should be established by meeting two of the following clinical, laboratory, or imaging criteria: abdominal pain and examination consistent with the disease, a serum amylase and/or lipase three times the upper limit of normal, and/or computed tomography, magnetic resonance imaging, or ultrasonography findings consistent with the disease.

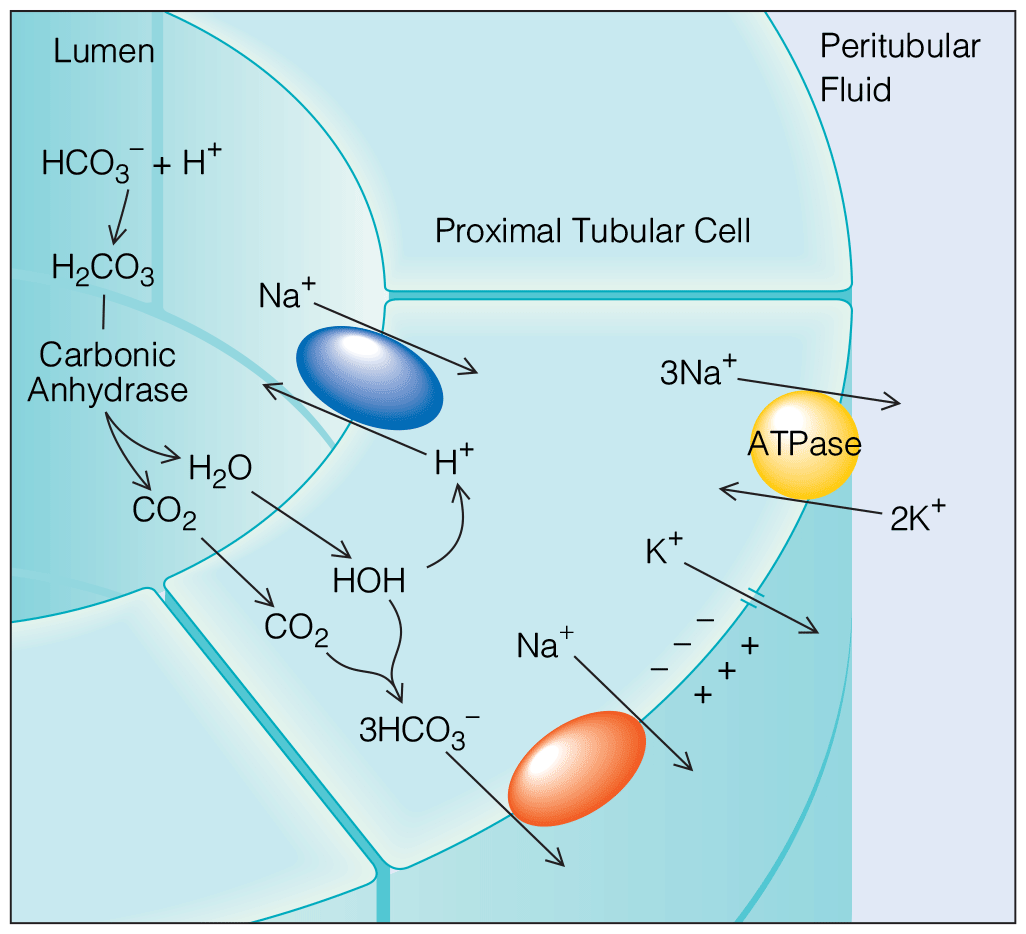
Disorders of Acid-Base and Potassium Balance
- Latest evidence-based management of potassium disorders.
- ATS guidelines for exercise-induced bronchoconstriction, asthma in the elderly, and asthma in the workplace
- ERS/ATS guideline for severe asthma discusses pharmacologic modalities of asthma management and bronchial thermoplasty.
- 2020 GINA practice guidelines no longer recommend treatment with SABA alone, without inhaled ICS. Recommend that all adults and adolescents with asthma should receive ICS-containing controller treatment.
- 2020 NAEPP practice guidelines delineating optimal treatment steps in adolescents and adults with asthma. This includes bronchial thermoplasty and immunotherapy.








.png)




















