
Physiologic and Anatomic Changes during Pregnancy
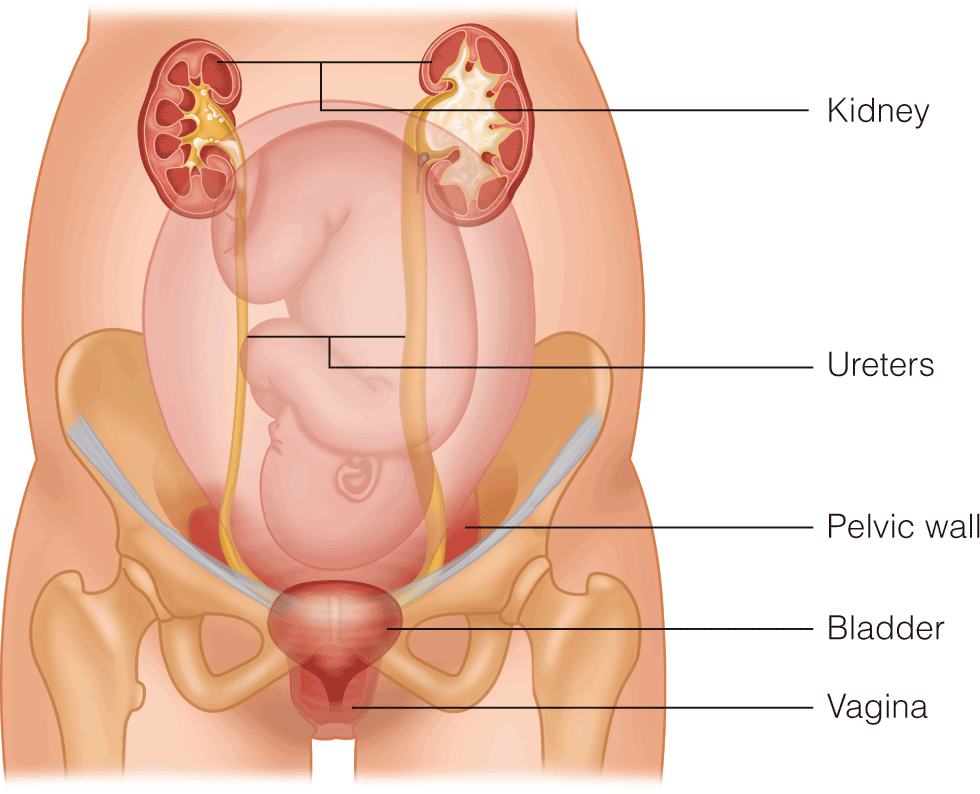
- A recent study using MRI demonstrated that left uterine displacement of at least 30° (not 15° as previously taught) is needed to relieve aortocaval compression.
- Pharyngeal volume decreases while airway Mallampati class increases throughout labor, which may contribute to increased risk of difficult intubation throughout labor.
- Thrombocytopenia commonly occurs in parturients, but the risk of spinal-epidural hematoma is exceedingly low.










.png)




















