
Coronaviruses: HCoV, SARS-CoV, MERS-CoV, and COVID-19
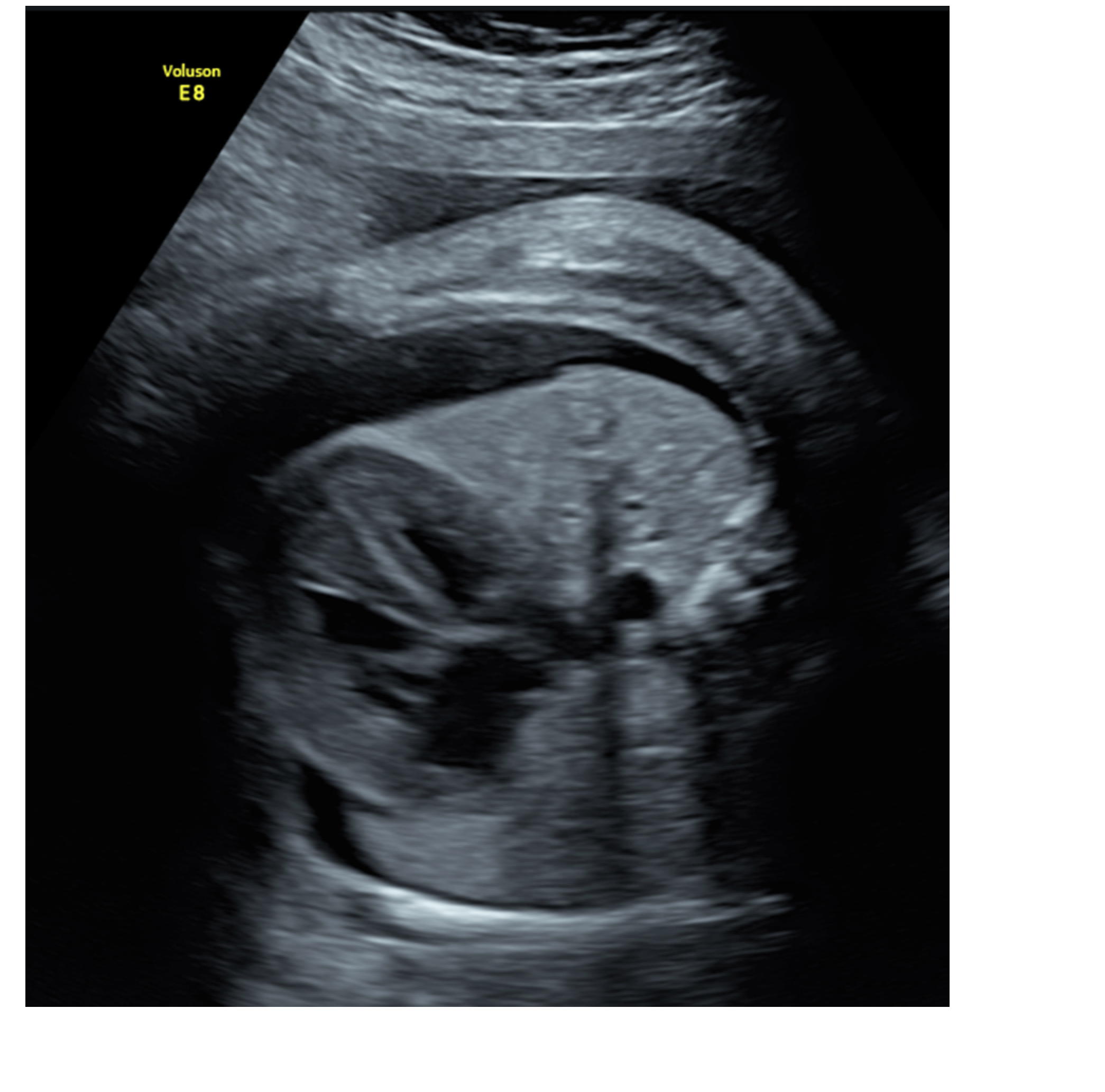
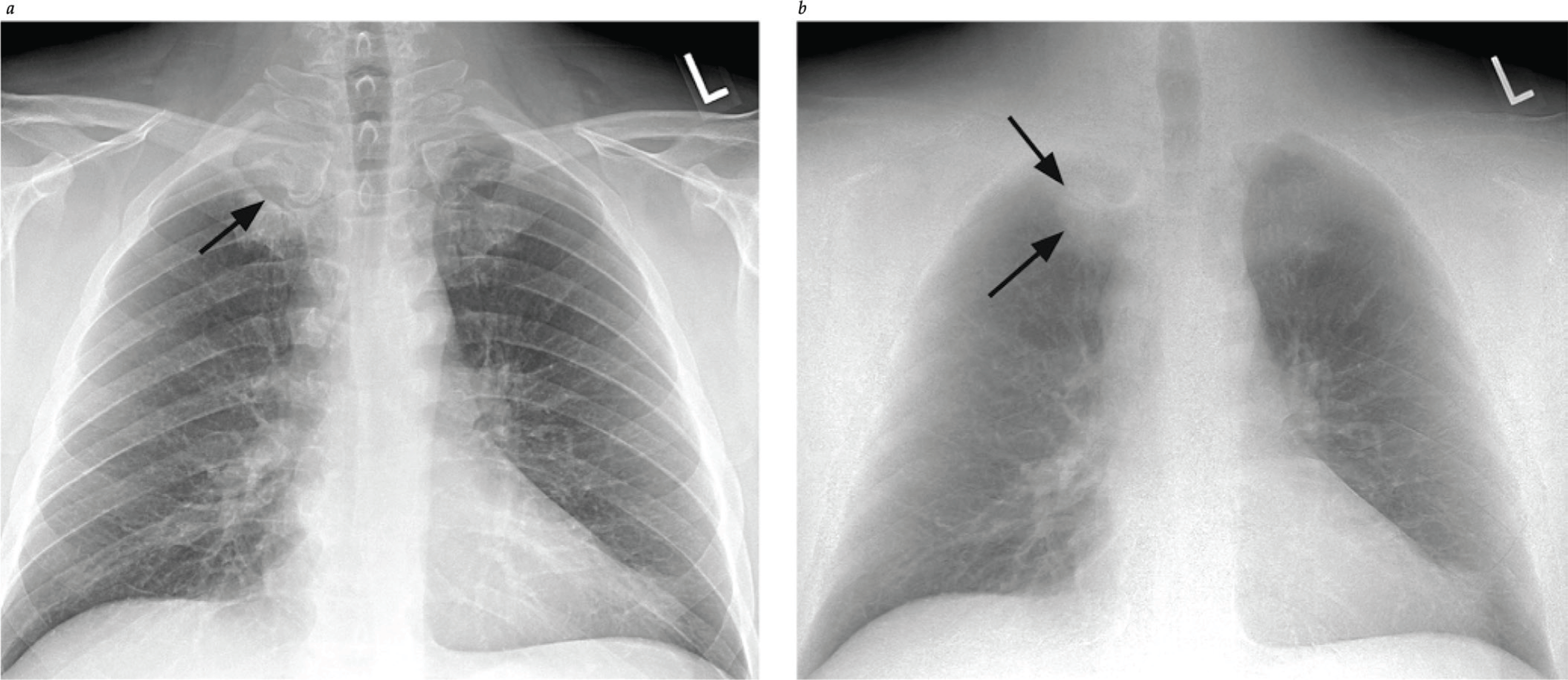
- Specific features on high resolution CT imaging for the more severe coronavirus syndromes are now accepted for clinical diagnosis in the appropriate context, followed by RT-PCR confirmation. This includes ground-glass opacity, with lower-lobe and bilateral involvement, and septal thickening. Other characteristics make diagnosis more or less likely.
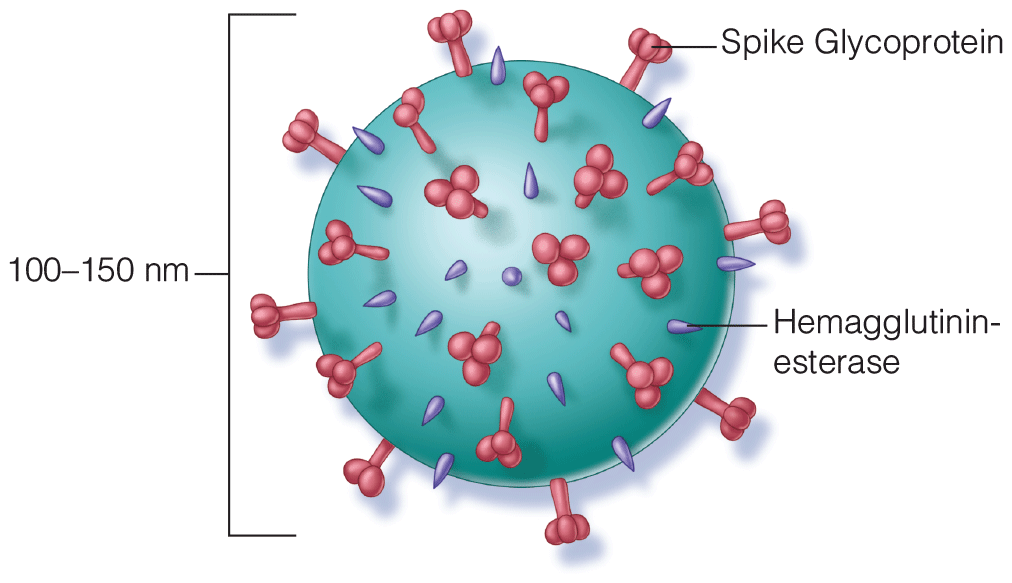
- Molecular studies of the evolution of the S protein affinity for COVID-19 allow more complete understanding of the mechanism of transmission and predisposing factors. These attachment proteins have highest affinity for ACE2 receptors on type II pneumocytes. What remains to be explained is the presence of virus in saliva, blood, urine and gastrointestinal tract: Are these potential modes of transmission?
- Two clinical trials have demonstrated promise for SARS-CoV-2 immunization; humoral and cellular immune responses are elicited. The preliminary data of these studies were published on July 20, 2020.














.png)
















