- Sepsis syndromes have been redefined (Sepsis-3 definitions) by international experts, based on sepsis mortality data extracted large administrative databases.
- National focus has turned to early identification of sepsis as a key determinant of outcomes. International critical care experts have recommended using the qSOFA criteria in the Emergency Department setting to identify sepsis risk in patients prior to obtaining diagnostics.
- The Center for Medicare and Medicaid Services (CMS) has added a sepsis quality measure (SEP-1) as a reporting requirement for all US hospital tied to Medicare & Medicaid reimbursement. This measure has increased awareness of sepsis performance and focused quality efforts on improvement.
- 2018 update to bundles to simplify to 1-hour bundle.
Latest Updates


- Sepsis syndromes have been redefined (Sepsis-3 definitions) by international experts, based on sepsis mortality data extracted large administrative databases.
- National focus has turned to early identification of sepsis as a key determinant of outcomes. International critical care experts have recommended using the qSOFA criteria in the Emergency Department setting to identify sepsis risk in patients prior to obtaining diagnostics.
- The Center for Medicare and Medicaid Services (CMS) has added a sepsis quality measure (SEP-1) as a reporting requirement for all US hospital tied to Medicare & Medicaid reimbursement. This measure has increased awareness of sepsis performance and focused quality efforts on improvement.
- 2018 update to bundles to simplify to 1-hour bundle.

- Sepsis syndromes have been redefined (Sepsis-3 definitions) by international experts, based on sepsis mortality data extracted large administrative databases.
- National focus has turned to early identification of sepsis as a key determinant of outcomes. International critical care experts have recommended using the qSOFA criteria in the Emergency Department setting to identify sepsis risk in patients prior to obtaining diagnostics.
- The Center for Medicare and Medicaid Services (CMS) has added a sepsis quality measure (SEP-1) as a reporting requirement for all US hospital tied to Medicare & Medicaid reimbursement. This measure has increased awareness of sepsis performance and focused quality efforts on improvement.
- 2018 update to bundles to simplify to 1-hour bundle.

Clinical Evaluation of Immigrant and Refugee Women
- Cultural sensitivity and openness is more important than cultural ‘competence’ when treating migrants from diverse backgrounds
- Guidelines are available for effective and appropriate use of qualified medical interpreters
- Mental health screening is not only to assess effects of prior trauma but to determine challenges in acculturation
- There is increasing recognition of the need for preventive counseling and chronic care in migrant women

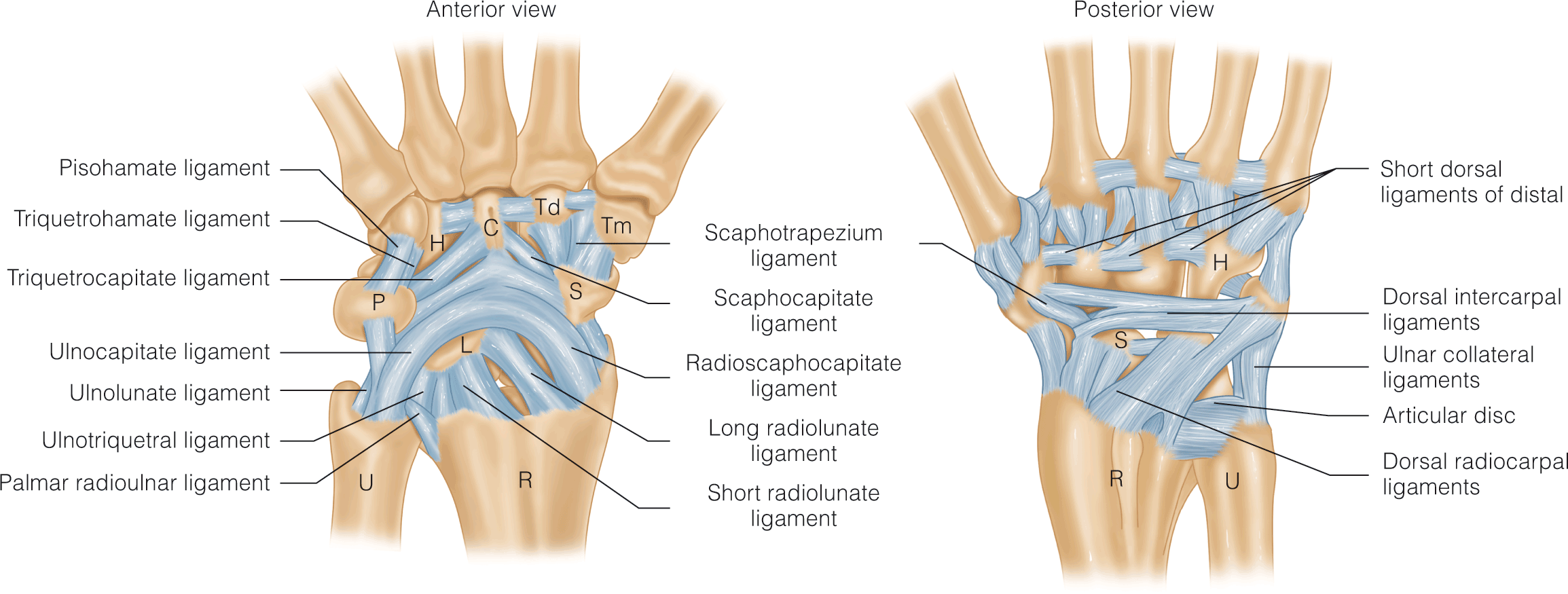
Hand and Wrist Ligament Injuries
- Arthroscopy technique continues to advance, remaining the ideal method for TFCC tear diagnosis and treatment.
- Novel SL ligament repair techniques are being developed (i.e., using FCR, palmaris tendons) with promising results.
- Data on conservative versus surgical care for fracture-dislocation of the CMCJ is mixed, requiring further study

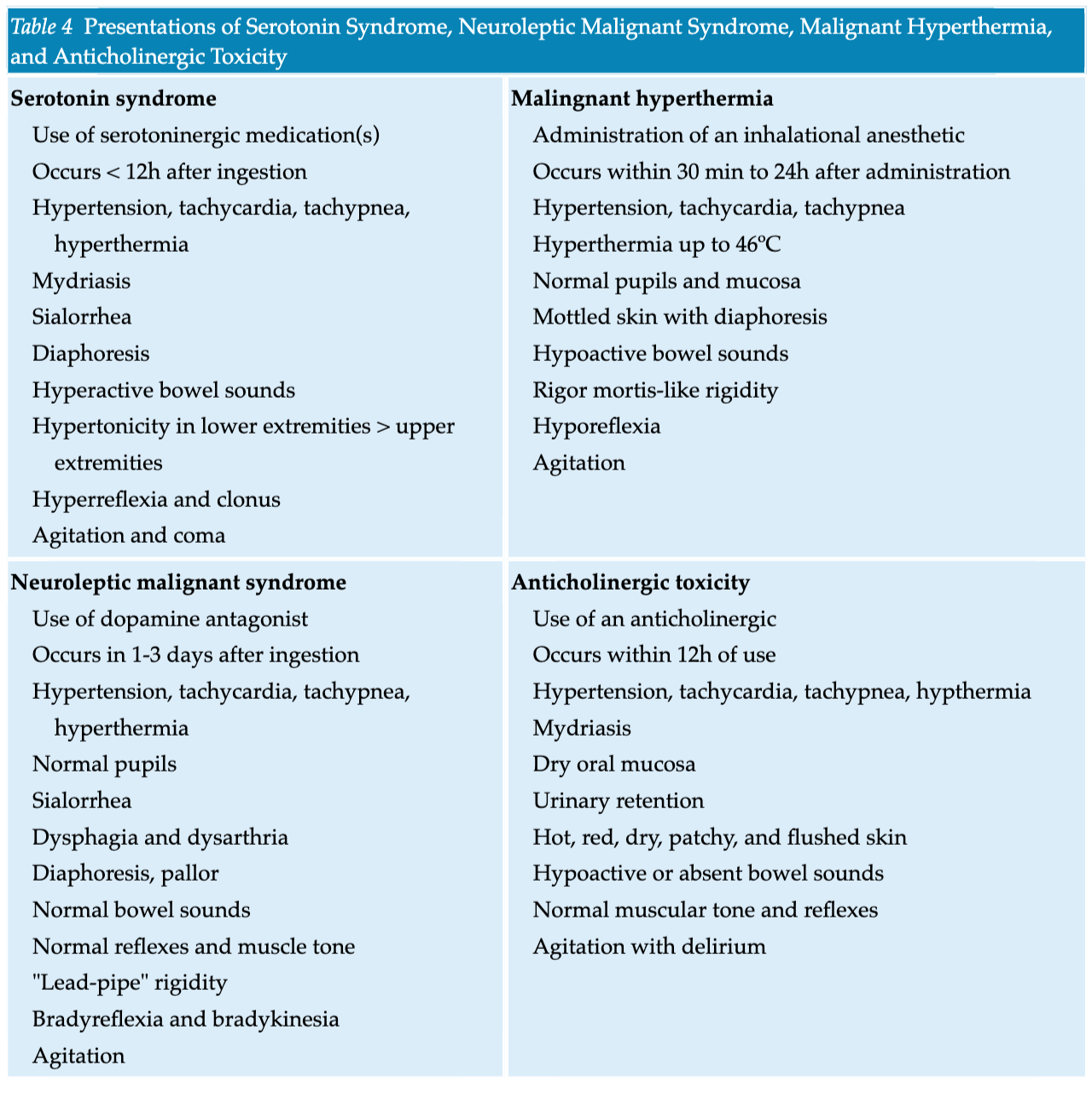
- Currently, there is a belief that the incidence of SS is congruent with the increasing number of serotoninergic agents prescribed and nutraceutical agents, such as St. John’s wort. In 2002, the Toxic Exposure Surveillance System reported 26,633 incidences of exposure to selective serotonin reuptake inhibitors (SSRIs) that caused significant adverse events in 7,349 patients, with a total of 93 deaths within the year.
- The Hunter Serotonin Toxicity Criteria are simpler, more sensitive, and more specific compared with Sternbach’s criteria. The Hunter criteria require a patient to have taken a serotoninergic agent and to meet one of the following conditions: spontaneous clonus; inducible clonus with agitation or diaphoresis; ocular clonus with agitation or diaphoresis; tremor with hyperreflexia; hypertonia with temperature above 38ºC (100.4°F) with ocular clonus or inducible clonus.
- In the setting of severe hyperthermia (temperature greater than 41°C [105.8°F]), immediate sedation with neuromuscular paralysis and intubation should occur to eliminate excessive muscle activity and thus prevent further complications. Nondepolarizing agents (e.g., vecuronium or atracurium) should be used for paralysis prior to intubation.
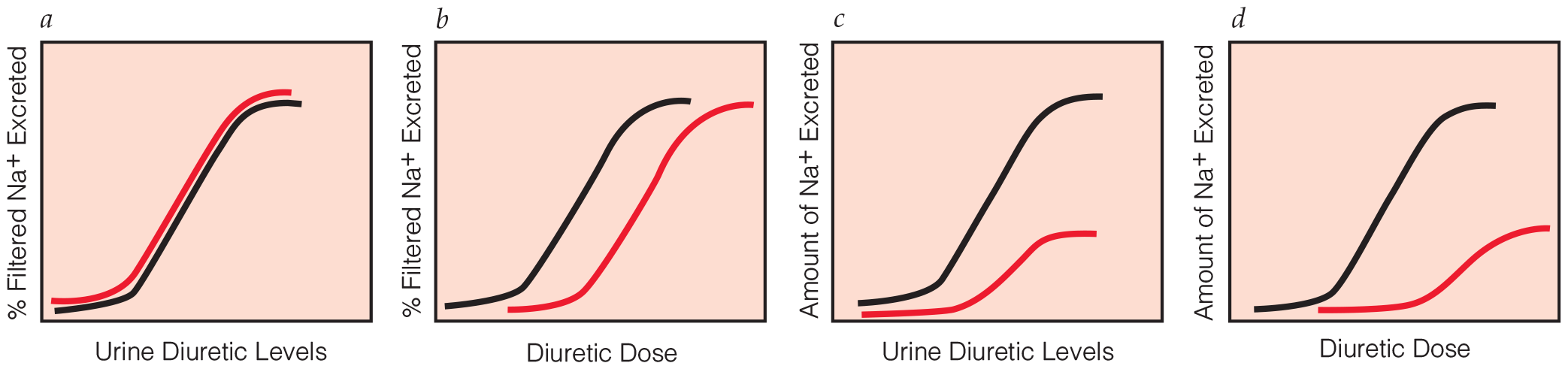
Disorders of Water and Sodium Balance: Hypernatremia
- Hydrochlorothiazide is not beneficial in treating ICU-acquired hypernatremia
- Hypernatremia after hypertonic saline irrigation is rare, but might cause severe complications
- Hypercalcemia induces targeted autophagic degradation of aquaporin-2 at the onset of nephrogenic diabetes insipidus
- Hypernatremia identified as new predictor of worse clinical outcomes after percutaneous endoscopic gastrostomy placement
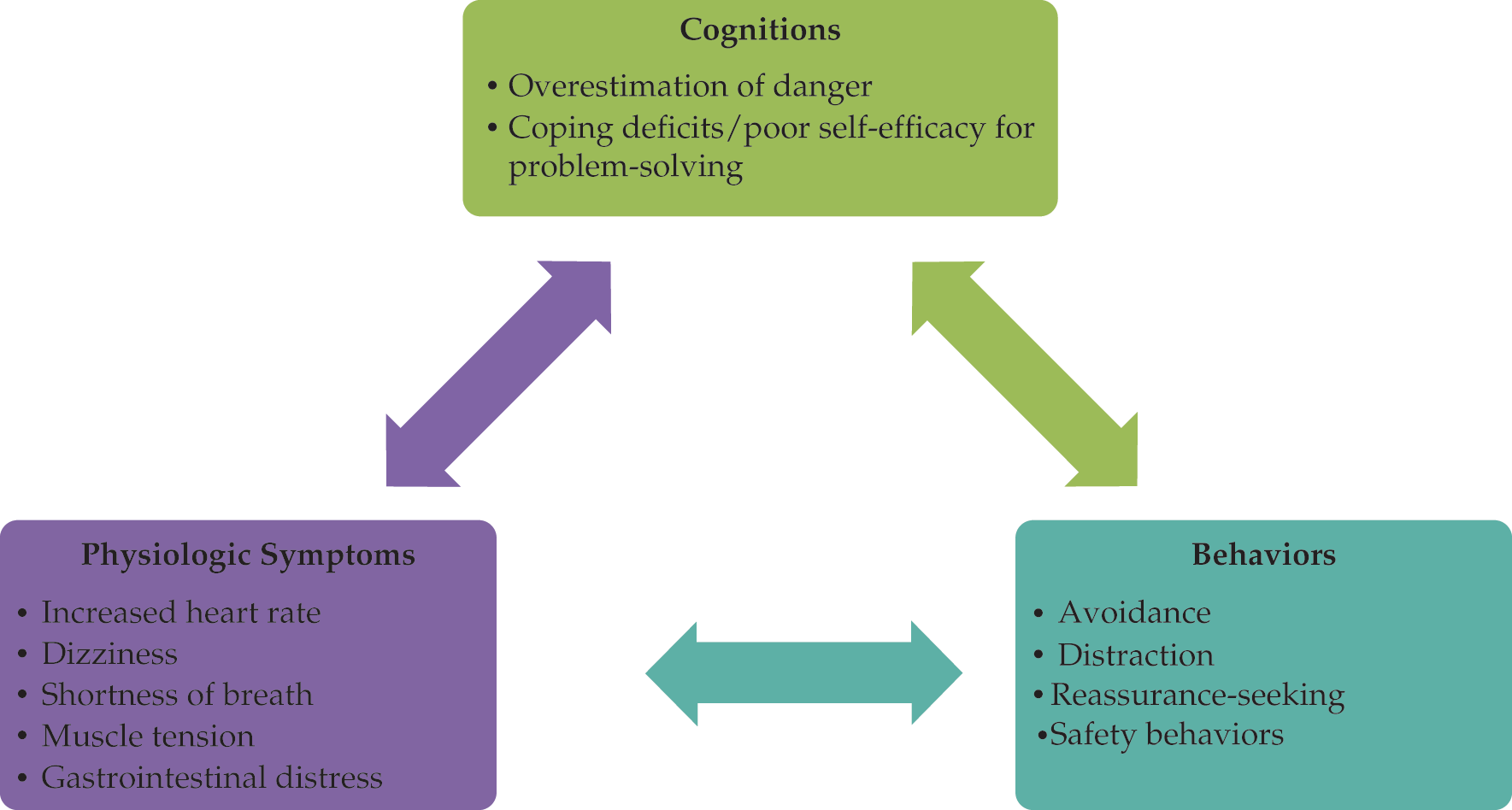
Clinical Management of Anxiety Disorders
- Identification of major anxiety disorders observed in adults according to the DSM-5
- Description of physiologic, cognitive, and behavioral components of anxiety and their relevance to diagnosis and treatment
- Review of cognitive-behavioral treatments and their efficacy for anxiety disorders in adults
- Review of pharmacologic treatments and their efficacy for anxiety disorders in adults









.png)
















