
Autoimmune Hepatitis/Overlap Syndromes
- Autoimmune hepatitis may have laboratory and histological features that resemble PBC or PSC, and PBC and PSC may have features of autoimmune hepatitis. These mixed clinical phenotypes constitute the overlap syndromes, and they may have a variable response to the conventional therapies used for each unmixed classical disease.
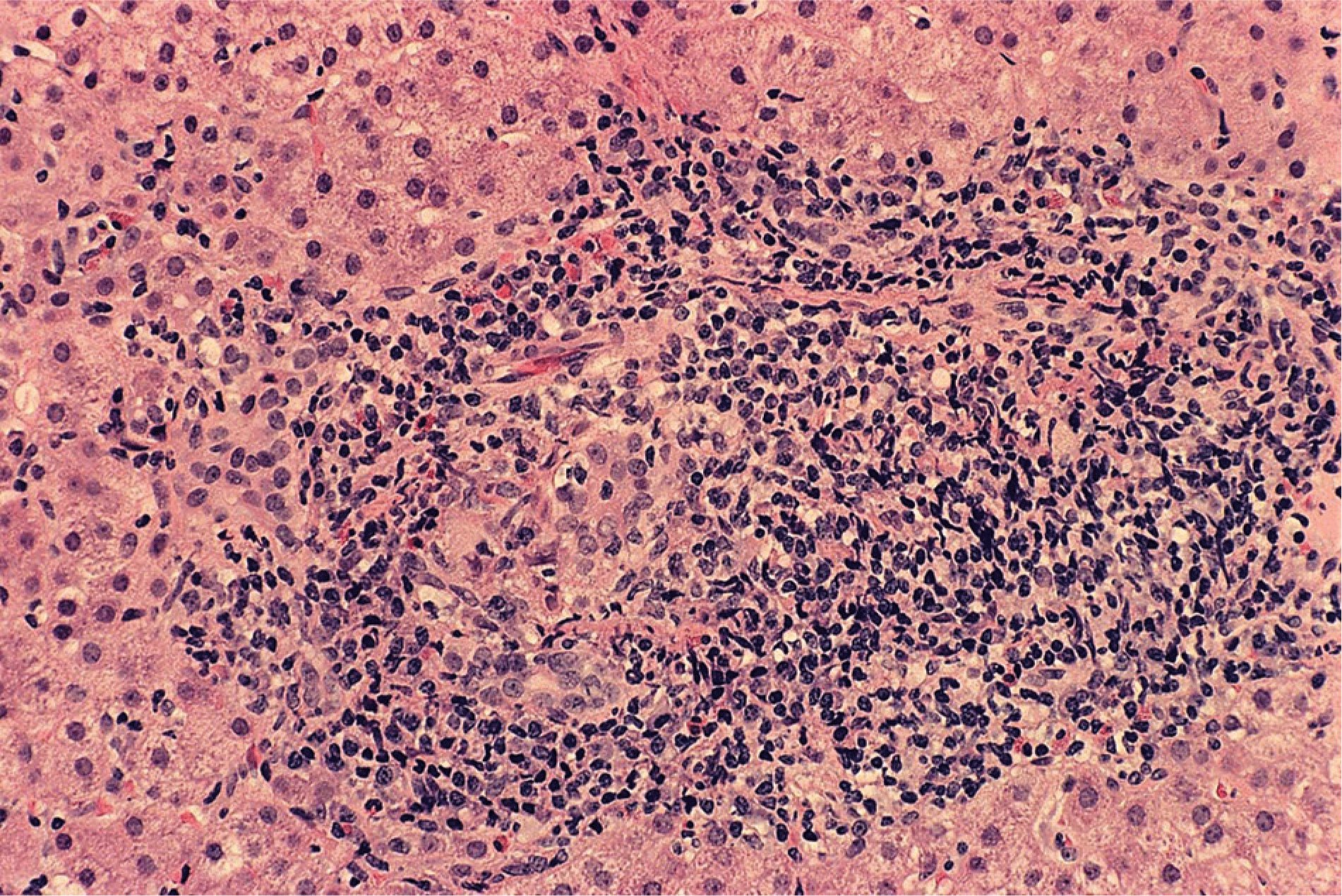
- Clinical judgment and expert interpretation of liver tissue are the principal bases for diagnosing the overlap syndromes, and incompatible manifestations of cholestasis (disproportionate serum AP and GGT elevations, destructive cholangitis or ductopenia in liver tissue) or liver inflammation (disproportionate serum AST and ALT elevations, interface hepatitis, and dense lymphoplasmacytic infiltration in liver tissue) are hallmarks of the diagnosis.
- Autoimmune hepatitis with cholestatic features that are unassociated with AMA or an abnormal cholangiography suggests the possibility of an overlap syndrome with AMA-negative PBC or small duct PSC.
- Therapy is guided by the predominant component of the overlap syndrome and consists mainly of prednisone or prednisolone, azathioprine, and low dose UDCA (13 to 15 mg/kg daily) in combination. Management strategies can be tailored to the individual patient and adjusted according to the response. High dose UDCA (28 to 30 mg/kg daily) should be avoided.
- Management of a nonresponse to the frontline regimen consists mainly of modifying the original treatment by adding corticosteroids or low dose UDCA if not present initially or considering the empirical use of mycophenolate mofetil as a substitute for azathioprine or a calcineurin inhibitor as a substitute for corticosteroids. Salvage drug therapies have had a limited clinical experience. Liver transplantation should be considered for features of liver failure.











.png)



















